The following is a report that I wrote for our Anaesthesia Equipment Committee at John Hunter Hospital in June 2017, after concerns were raised about differences in performance of different filter types, and the possible cross-contamination risks resulting from this.
Introduction
It has long been known that breathing circuits are a potential source of cross infection between patients . Of particular concern are hepatitis C and tuberculosis . Eliminating this risk altogether seems unlikely, but there is ongoing debate about how best to reduce the risk, while also being conscious of financial and environmental concerns . The use of breathing system filters (BSF) is one approach that has tried to address some of the concerns, and the presumption that they protect the anaesthetic circuit from contamination by the patient and vice versa has led to the widespread adoption of BSFs as a way to reduce cost and waste by facilitating the reuse of the same circuit for multiple patients . However the practice is not universal , and no BSF is 100% effective at preventing contamination . Furthermore, as with any piece of medical equipment, the risks associated with the use of BSFs need to be considered along with their benefits . Many manufacturers now produce circuits that are approved for use for up to 1 week as long as a new BSF is used for each patient . This is the current policy at John Hunter, with the proviso that the circuit is changed immediately if it is visibly soiled, has been used for a patient with a multidrug-resistant organism, or is excessively wet. If we assume this practice will continue, then the question that needs to be answered is which filter will best protect the circuit from contamination, and that question is the main focus of this report.
Summary
Features of an ideal breathing system filter (BSF)
- Good airborne and liquid-borne filtration performance
- Good moisture output (where HME function is desired)
- High liquid penetration pressure
- Low dead space
- Low resistance to flow, including when wet
- Low weight
- Transparent housing
- No sharp corners or protrusions
- Attachment for gas monitoring, with a brightly coloured, tethered cap
- Low cost
Key Safety Points
- Pleated mechanical filters reduce the risk of contamination of the machine side of the filter more effectively than electrostatic filters
- Risk of contamination of the machine side of the BSF is increased if there are high ventilatory pressures (eg coughing)
- The BSF should be considered as a contributing factor whenever there is difficulty ventilating a patient
- BSFs are at higher risk of obstruction if airway secretions are increased, nebulised drugs are given, a humidified circuit is used, or the device is below the patient’s airway (eg prone)
- Caps covering the gas monitoring port should be tethered to the filter housing
Definitions and abbreviations
-
- BSF: Breathing System Filter
- HME: Heat & Moisture Exchange
- HMEF: Heat & Moisture Exchange Filter
- hPa: hectopascal » 1 cm H2O
- Two main categories of BSF (for a good comparison see Wilkes, 2002 )
- Electrostatic
- Mechanical (aka pleated hydrophobic)
Recommendation
Where an anaesthetic circuit will be used for multiple patients, the circuit should be protected by a new breathing system filter for each patient. This filter should have a liquid penetration pressure of greater than 60 hPa, or at least 20 hPa above the maximum ventilation pressure in the anaesthetic system. Currently, this requires the use of a pleated hydrophobic mechanical filter. The cap covering the gas-sampling port should be tethered to the filter housing.
Report
The risk of cross-contamination of patients via anaesthetic equipment rose to prominence following a series of hepatitis C cases in 1993 where the anaesthetic circuit was the most likely fomite . Since then BSFs have commonly been included in infection-control policies for anaesthesia, but there are exceptions. For example, in the USA they are only explicitly recommended when a patient has tuberculosis . Unfortunately, even when a BSF is recommended, the guidelines are often lacking in detail about what features and specifications are required, or even desirable. Rather, they just state that one should be used. There is also ongoing disagreement over how high the risk of cross-contamination is in the absence of a BSF, as well as how much this risk is reduced when one is present .
But once the decision to use a BSF has been made, the question then becomes, “Which one?”. While all the properties of a filter will influence this decision, there appears to be a factor of particular relevance to the question of which BSF will best protect the circuit from contamination if you intend to use it for another patient. It is related to a significant difference inherent in the design of the two broad categories of filters, namely “mechanical” and “electrostatic”. The issue of concern is the pressure required to force liquid through the filter, and it was an observation of this difference by an anaesthetic staff member at John Hunter that triggered the discussion that prompted this report.
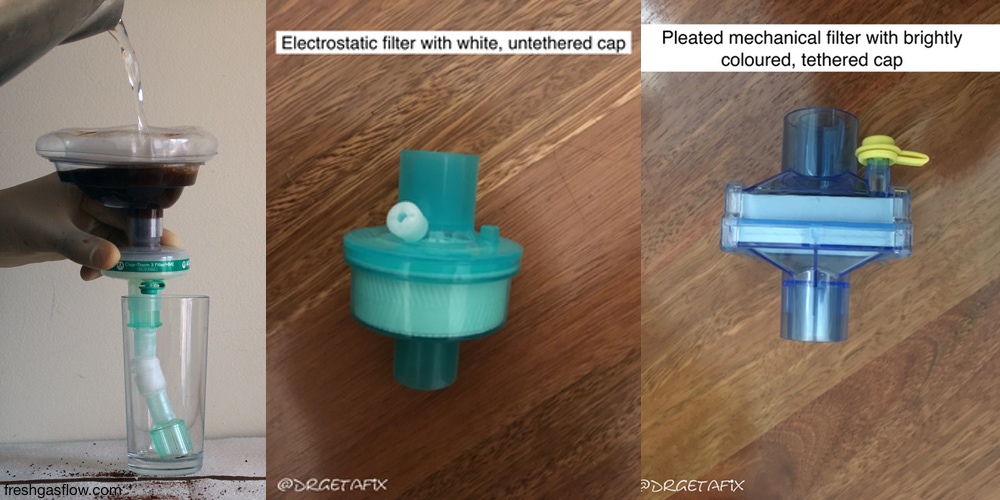
According to BSF manufacturers, both classes have comparable filtration efficiencies, however their testing methods differ, making it difficult to compare products using this data. However, when compared using standardised test conditions, mechanical filters will generally outperform electrostatic filters , and there is some evidence that mechanical filters are more effective at preventing contamination of the circuit , especially by viruses . This difference is even more pronounced in wet conditions. As a BSF gets wet the resistance to flow, and therefore airway pressure, tends to increase . This rise in pressure is greatest in electrostatic BSFs, and as more liquid is added, the pressure continues to rise until the filter is breached and liquid is ejected through it. Often, once the BSF has been breached, liquid can pass through it freely . Of particular concern is the fact that this ejection pressure is usually well within the range of airway pressures experienced during anaesthesia, especially if the patient coughs, or mechanical ventilation is used . If liquid does penetrate the filter, then any microbes in the liquid will go with it, thus contaminating the circuit and putting the next patient at risk of infection. As for mechanical filters, the pressure increase observed with the addition of liquid is less, and a greater volume of liquid needs to be added for the pressure rise to occur. The pressure required to breach a mechanical filter is also much higher, and is usually well outside the range of airway pressures experienced clinically, and when it is breached, liquid tends to flow through more slowly than with an electrostatic filter . However, this higher breakthrough pressure means that, if enough liquid is added, complete obstruction can occur. This prompted one author to raise the question as to whether it is clinically preferable to prevent passage of liquid secretions and risk occlusion or to allow the passage of such fluids and risk contamination . It should be noted however that airway obstruction due to BSFs is not limited to mechanical filters , and it could be argued that the readily apparent risk to patient safety caused by filter occlusion is “preferable” to the potentially undetectable infection risk caused by liquid contamination of the circuit. This latter concern is heightened because it is often harder to detect accumulation of water in electrostatic filters than in mechanical ones, and given that the same circuit is used for up to seven days, a contaminated circuit will potentially expose dozens of patients to this increased risk of infection. Furthermore, once the circuit has been contaminated, the anaesthetic machine itself is exposed to an increased risk of contamination, and if that occurs, exposure of subsequent patients to the risk of cross-infection will remain even after the circuit is changed. Of course, in order for a subsequent patient to be exposed to any contaminant, some microbes from the circuit or the machine will need to pass back through the new filter, and while this double transfer seems unlikely , it nonetheless represents a latent condition that may one day contribute to patient harm.
This significant difference between mechanical and electrostatic filters has led to the recommendation that mechanical filters be used in preference to electrostatic filters, especially with circle breathing systems utilising low flows where condensation in the circuit is common . The German Society for Anaesthesiology and Intensive Care has recognised this issue and has actually specified the pressures that a BSF must be able to withstand before being breached , which is a de-facto recommendation for a mechanical filter given their superior performance in that regard.
So, if the primary reason for the use of a BSF is to allow reuse of the circuit for multiple patients, then a mechanical filter will provide the best defence against contamination of equipment, and therefore against cross-contamination between patients. In general, mechanical filters are more expensive than electrostatic filters, however this cost will be more than recovered by the savings achieved by reusing a circuit for multiple patients.
Consideration also needs to be given to the role that BSFs can play in warming and humidifying inspired gases, i.e. heat and moisture exchange (HME). This is important as the upper airways, which normally warm and humidify inspired air, have been bypassed, and delivery of cold, dry air to the lower respiratory tract for a prolonged period can cause significant problems . Some BSFs have a degree of intrinsic HME capability, while others will have an additional HME component added, or there will be some modification made to the filtration component to improve its HME performance . If a BSF has both HME and filtration functions, then, not surprisingly, it is termed an HMEF. Wilkes has suggested a minimum target for moisture output of 20 g.m3 for short-duration use in anaesthesia, and 30 g.m-3 for longer term ICU ventilation . Unfortunately, a lot of manufacturers haven’t measured or don’t provide the moisture output of their products, and even when they do, it needs to be remembered that the HME performance will be affected by tidal volumes, duration of use, size, as well as the temperature and humidity of expired air, so there can be some discrepancy between in vitro and in vivo performance . It should also be noted that a circle breathing system can provide a significant degree of warming and humidification to the air passing through it, especially at low flows , as a result of the exothermic, water producing reaction between the carbon dioxide and the absorbent.
Finally, there are a number of potential complications and safety concerns that need to be considered, and that practitioners need to be mindful of. Any kind of BSF will provide an additional point of potential circuit disconnection, and as previously alluded to, an additional point of airway obstruction , including by foreign bodies . There have also been reports of BSFs affecting ventilator triggering and alarms . These points are particularly pertinent given that BSFs are often not visible or easily accessible because they are underneath drapes, or close to the surgical field. Also, the risk of BSF obstruction is increased whenever the device is below the level of the patient’s airway (e.g. prone surgery), as then any liquid in the circuit will flow into the filter . There is also the concern, depending on the size, weight, shape and location of the filter, that they can exert excessive pressure on the patient’s skin, or cause traction or torque of the circuit, especially if they have square corners or parts protruding from the housing. Particular care also needs to be taken with patients who are coughing, have significant airway secretions or pulmonary oedema, and it is generally recommended that a BSF should not be used if there is active humidification of the circuit, or nebulised medications are being given. While these concerns are common to all BSFs, there are some features to look for that may decrease these risks, or make it easier to identify problems. For example, using a filter with transparent housing will make it easier to identify fluid accumulation or foreign bodies. There are also BSFs available with rounded edges, and if possible, it would be advisable to use a filter where the gas sampling port has a tethered cap to reduce the risk of the cap falling into the breathing circuit and causing obstruction . In addition to this, if the packaging and caps are brightly coloured (increasing their visibility), this might also decrease the risk of obstruction, or at least make identification of the cause easier .
Conclusion
While some questions remain unanswered or would benefit from further clarification, it is clear that mechanical BSFs outperform electrostatic versions when it comes to protecting the anaesthetic circuit from contamination. While some consideration needs to be given to other features such as moisture output, cost, dead space etc, it would seem that the best approach would be to use these secondary considerations as a way to discriminate between the multiple varieties of mechanical filters, which are the most appropriate option to address the primary consideration of preventing cross-infection between patients.
{4088554:UCNRZPQA},{4088554:QQZ6BN6J},{4088554:38CKDQE3},{4088554:DXJJDAAF};{4088554:K4VDA9I4};{4088554:BVVF4DZG},{4088554:MHSHAUVV},{4088554:IS5AK4QN};{4088554:67AXM25W},{4088554:K7E6M3V2};{4088554:AN6U2CDN};{4088554:449K8DEF};{4088554:R2EHRWFW};{4088554:K4VDA9I4};{4088554:99U6ZXDG};{4088554:38CKDQE3};{4088554:S7FG4K9G},{4088554:X34P9ZBW},{4088554:47MR3BBE};{4088554:AN6U2CDN},{4088554:AQDTDVKA};{4088554:AN6U2CDN},{4088554:7XWUPGXD},{4088554:8PQEAMI4},{4088554:4MCTWJUW};{4088554:5W5IH8BX};{4088554:4DEFM9MT};{4088554:8TNBEWCZ};{4088554:8TNBEWCZ},{4088554:K4VDA9I4};{4088554:42G52X47};{4088554:8TNBEWCZ},{4088554:SZ27T9S9},{4088554:N4V8G47Z},{4088554:C6QJGDNZ};{4088554:IXVUZJA5},{4088554:Z8ZWE3HG};{4088554:5W5IH8BX};{4088554:FEMZXWSF};{4088554:5W5IH8BX};{4088554:HENVB463};{4088554:UWCDZM7F},{4088554:H67GCR94};{4088554:Z8ZWE3HG};{4088554:ATDHSUUF};{4088554:FEMZXWSF},{4088554:R3WTJP7N};{4088554:S7FG4K9G};{4088554:FEMZXWSF};{4088554:U7T48XRT},{4088554:4DEFM9MT};{4088554:FEMZXWSF};{4088554:GHHP2KXI};{4088554:FEMZXWSF},{4088554:W39AC5HR},{4088554:UEGVW8ZN};{4088554:UWCDZM7F},{4088554:H67GCR94},{4088554:V5C645BH},{4088554:DI8SANXZ};{4088554:DI8SANXZ};{4088554:VZ5EU488};{4088554:SFNZ2452};{4088554:UEGVW8ZN},{4088554:QIN8NDBI};{4088554:WM5RDKDU},{4088554:PW24ZVS2}
nature
default
asc
0
427
%7B%22status%22%3A%22success%22%2C%22updateneeded%22%3Afalse%2C%22instance%22%3Afalse%2C%22meta%22%3A%7B%22request_last%22%3A350%2C%22request_next%22%3A50%2C%22used_cache%22%3Atrue%7D%2C%22data%22%3A%5B%7B%22key%22%3A%22QHC3GQDN%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Rae%20et%20al.%22%2C%22parsedDate%22%3A%222020%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BRae%2C%20A.%2C%20Provan%2C%20D.%2C%20Aboelssaad%2C%20H.%20%26amp%3B%20Alexander%2C%20R.%20A%20manifesto%20for%20Reality-based%20Safety%20Science.%20%26lt%3Bi%26gt%3BSafety%20Science%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B126%26lt%3B%5C%2Fb%26gt%3B%2C%20104654%20%282020%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22A%20manifesto%20for%20Reality-based%20Safety%20Science%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Andrew%22%2C%22lastName%22%3A%22Rae%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22David%22%2C%22lastName%22%3A%22Provan%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Hossam%22%2C%22lastName%22%3A%22Aboelssaad%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Rob%22%2C%22lastName%22%3A%22Alexander%22%7D%5D%2C%22abstractNote%22%3A%22In%20the%20%5Cufb01eld%20of%20safety%20science%2C%20we%20have%20stopped%20competing%20empirically.%20The%20theorists%20%5Cufb01ght%20each%20other%20with%20keynotes%20and%20editorials%2C%20the%20empiricists%20tinker%20within%20the%20boundaries%20of%20existing%20theory%2C%20and%20the%20practitioners%20use%20neither%20theory%20nor%20evidence%20to%20determine%20their%20activities.%22%2C%22date%22%3A%2206%5C%2F2020%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.ssci.2020.104654%22%2C%22ISSN%22%3A%2209257535%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Flinkinghub.elsevier.com%5C%2Fretrieve%5C%2Fpii%5C%2FS0925753520300515%22%2C%22collections%22%3A%5B%22Z3QQKF3J%22%5D%2C%22dateModified%22%3A%222020-02-17T00%3A58%3A39Z%22%7D%7D%2C%7B%22key%22%3A%22ND529MV5%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Salmon%20et%20al.%22%2C%22parsedDate%22%3A%222020%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BSalmon%2C%20P.%20M.%20%26lt%3Bi%26gt%3Bet%20al.%26lt%3B%5C%2Fi%26gt%3B%20The%20big%20picture%20on%20accident%20causation%3A%20A%20review%2C%20synthesis%20and%20meta-analysis%20of%20AcciMap%20studies.%20%26lt%3Bi%26gt%3BSafety%20Science%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B126%26lt%3B%5C%2Fb%26gt%3B%2C%20104650%20%282020%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22The%20big%20picture%20on%20accident%20causation%3A%20A%20review%2C%20synthesis%20and%20meta-analysis%20of%20AcciMap%20studies%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Paul%20M.%22%2C%22lastName%22%3A%22Salmon%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Adam%22%2C%22lastName%22%3A%22Hulme%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Guy%20H.%22%2C%22lastName%22%3A%22Walker%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Patrick%22%2C%22lastName%22%3A%22Waterson%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Elise%22%2C%22lastName%22%3A%22Berber%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Neville%20A.%22%2C%22lastName%22%3A%22Stanton%22%7D%5D%2C%22abstractNote%22%3A%22As%20AcciMap%20is%20now%20arguably%20the%20most%20popular%20accident%20analysis%20method%20in%20the%20peer-reviewed%20literature%2C%20there%20are%20key%20learnings%20to%20be%20taken%20from%20reviewing%20and%20synthesising%20published%20AcciMap%20analyses.%20In%20particular%2C%20the%20extent%20to%20which%20the%20network%20of%20contributory%20factors%20underpinning%20accidents%20is%20consistent%20across%20safety%20critical%20domains.%20This%20study%20reviewed%20and%20synthesised%2023%20AcciMap%20analyses%20published%20in%20the%20peer-reviewed%20literature.%20Contributory%20factors%20and%20relationships%20were%20extracted%20and%20thematically%20coded%20to%20form%20a%20single%20multi-domain%2C%20multi-incident%20AcciMap.%20The%20resulting%20AcciMap%20contains%205587%20contributory%20factors%20spanning%20seventy-nine%20distinct%20contributory%20factor%20types.%20The%20findings%20reveal%20a%20set%20of%20generic%20contributory%20factors%20that%20consistently%20play%20a%20role%20in%20major%20accidents%20regardless%20of%20domain.%20Additionally%2C%20contributory%20factors%20previously%20only%20associated%20with%20sharp-end%20human%20operators%20are%2C%20in%20fact%2C%20prevalent%20across%20multiple%20levels%20of%20accident%20systems.%20The%20implications%20of%20these%20findings%20for%20accident%20theory%20and%20accident%20analysis%20and%20prevention%20activities%20are%20discussed.%20For%20future%20AcciMap%20analyses%20it%20is%20recommended%20that%20the%20contributory%20factor%20classification%20scheme%20developed%20in%20the%20present%20study%20is%20used%20to%20support%20the%20identification%20and%20classification%20of%20contributory%20factors.%20In%20addition%2C%20further%20education%20for%20analysts%20on%20the%20systems%20thinking%20perspective%20on%20accident%20causation%20is%20recommended.%22%2C%22date%22%3A%2206%5C%2F2020%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.ssci.2020.104650%22%2C%22ISSN%22%3A%2209257535%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Flinkinghub.elsevier.com%5C%2Fretrieve%5C%2Fpii%5C%2FS0925753520300473%22%2C%22collections%22%3A%5B%22Z3QQKF3J%22%5D%2C%22dateModified%22%3A%222020-02-17T00%3A58%3A19Z%22%7D%7D%2C%7B%22key%22%3A%22IUJ7CC3P%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Zippel%20et%20al.%22%2C%22parsedDate%22%3A%222014%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BZippel%2C%20C.%2C%20B%26%23xF6%3Brgers%2C%20A.%2C%20Weitzel%2C%20A.%20%26amp%3B%20Bohnet-Joschko%2C%20S.%20Many%20critical%20incidents%20could%20be%20avoided%20by%20preanaesthesia%20equipment%20checks%3A%20Lessons%20for%20high%20reliability%20organisations.%20%26lt%3Bi%26gt%3BEuropean%20Journal%20of%20Anaesthesiology%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B31%26lt%3B%5C%2Fb%26gt%3B%2C%20289%26%23x2013%3B291%20%282014%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Many%20critical%20incidents%20could%20be%20avoided%20by%20preanaesthesia%20equipment%20checks%3A%20Lessons%20for%20high%20reliability%20organisations%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Claus%22%2C%22lastName%22%3A%22Zippel%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Andr%5Cu00e9%22%2C%22lastName%22%3A%22B%5Cu00f6rgers%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Andreas%22%2C%22lastName%22%3A%22Weitzel%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Sabine%22%2C%22lastName%22%3A%22Bohnet-Joschko%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2205%5C%2F2014%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1097%5C%2FEJA.0000000000000054%22%2C%22ISSN%22%3A%220265-0215%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fcontent.wkhealth.com%5C%2Flinkback%5C%2Fopenurl%3Fsid%3DWKPTLP%3Alandingpage%26an%3D00003643-201405000-00011%22%2C%22collections%22%3A%5B%22HF2N89AI%22%5D%2C%22dateModified%22%3A%222020-02-16T12%3A21%3A45Z%22%7D%7D%2C%7B%22key%22%3A%22LAPINXSW%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Zippel%20et%20al.%22%2C%22parsedDate%22%3A%222014-05%22%2C%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BZippel%2C%20C.%2C%20Borgers%2C%20A.%2C%20Weitzel%2C%20A.%20%26amp%3B%20Bohnet-Joschko%2C%20S.%20Many%20critical%20incidents%20could%20be%20avoided%20by%20preanaesthesia%20equipment%20checks%3A%20Lessons%20for%20high%20reliability%20organisations.%26%23xA0%3B%20%5BLetter%5D.%20%26lt%3Bi%26gt%3BJournal%20of%20Anaesthesiology%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B31%26lt%3B%5C%2Fb%26gt%3B%2C%20289%26%23x2013%3B291%20%282014%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Many%20critical%20incidents%20could%20be%20avoided%20by%20preanaesthesia%20equipment%20checks%3A%20Lessons%20for%20high%20reliability%20organisations.%20%20%5BLetter%5D%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Claus%22%2C%22lastName%22%3A%22Zippel%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Andre%22%2C%22lastName%22%3A%22Borgers%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Andreas%22%2C%22lastName%22%3A%22Weitzel%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Sabine%22%2C%22lastName%22%3A%22Bohnet-Joschko%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222014%20May%22%2C%22language%22%3A%22English.%22%2C%22DOI%22%3A%2210.1097%5C%2FEJA.0000000000000054%22%2C%22ISSN%22%3A%220265-0215%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22HF2N89AI%22%5D%2C%22dateModified%22%3A%222020-02-16T12%3A21%3A16Z%22%7D%7D%2C%7B%22key%22%3A%22SKYH3IZ4%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Wilkes%20et%20al.%22%2C%22parsedDate%22%3A%222011%22%2C%22numChildren%22%3A2%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BWilkes%2C%20A.%20R.%2C%20Pandit%2C%20J.%20J.%20%26amp%3B%20O%26%23x2019%3BSullivan%2C%20E.%20The%20history%20of%20anaesthetic%20equipment%20evaluation%20in%20the%20United%20Kingdom%3A%20lessons%20for%20developing%20future%20strategy.%20%26lt%3Bi%26gt%3BAnaesthesia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B66%26lt%3B%5C%2Fb%26gt%3B%2C%2034%26%23x2013%3B39%20%282011%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22The%20history%20of%20anaesthetic%20equipment%20evaluation%20in%20the%20United%20Kingdom%3A%20lessons%20for%20developing%20future%20strategy%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A.%20R.%22%2C%22lastName%22%3A%22Wilkes%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22J.%20J.%22%2C%22lastName%22%3A%22Pandit%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22E.%22%2C%22lastName%22%3A%22O%5Cu2019Sullivan%22%7D%5D%2C%22abstractNote%22%3A%22Recent%20guidance%20published%20by%20the%20Association%20of%20Anaesthetists%20of%20Great%20Britain%20and%20Ireland%20encourages%20the%20purchase%20of%20equipment%20based%20on%20evidence%20of%20safety%20and%20performance.%20For%20many%20years%2C%20evidence%20of%20the%20safety%20and%20performance%20of%20anaesthetic%20equipment%20was%20published%20by%20various%20government%20departments%20and%20agencies.%20However%2C%20these%20schemes%20were%20gradually%20eroded%20over%20time%20such%20that%20many%20devices%20entered%20the%20market%20with%20little%20or%20no%20clinical%20evidence%20of%20their%20efficacy.%20This%20recently%20led%20to%20the%20Difficult%20Airway%20Society%5Cu2019s%20issuing%20guidance%20to%20its%20members%20on%20how%20best%20to%20select%20new%20airway%20devices%3B%20guidance%20that%20was%20based%20on%20the%20available%20evidence.%20This%20article%20provides%20a%20short%20history%20of%20the%20evaluation%20of%20anaesthetic%20equipment%20in%20the%20United%20Kingdom.%22%2C%22date%22%3A%222011%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1111%5C%2Fj.1365-2044.2011.06932.x%22%2C%22ISSN%22%3A%221365-2044%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fonlinelibrary.wiley.com%5C%2Fdoi%5C%2Fabs%5C%2F10.1111%5C%2Fj.1365-2044.2011.06932.x%22%2C%22collections%22%3A%5B%22MXVKNACE%22%5D%2C%22dateModified%22%3A%222020-02-16T12%3A16%3A16Z%22%7D%7D%2C%7B%22key%22%3A%228RE4SYLL%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Cook%20et%20al.%22%2C%22parsedDate%22%3A%222019%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BCook%2C%20T.%20M.%20%26lt%3Bi%26gt%3Bet%20al.%26lt%3B%5C%2Fi%26gt%3B%20Multicentre%20clinical%20simulation%20evaluation%20of%20the%20ISO%2080369-6%20neuraxial%20non-Luer%20connector.%20%26lt%3Bi%26gt%3BAnaesthesia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B74%26lt%3B%5C%2Fb%26gt%3B%2C%20619%26%23x2013%3B629%20%282019%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Multicentre%20clinical%20simulation%20evaluation%20of%20the%20ISO%2080369-6%20neuraxial%20non-Luer%20connector%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22T.%20M.%22%2C%22lastName%22%3A%22Cook%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A.%22%2C%22lastName%22%3A%22Wilkes%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22P.%20Bickford%22%2C%22lastName%22%3A%22Smith%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22L.%22%2C%22lastName%22%3A%22Dorn%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22M.%22%2C%22lastName%22%3A%22Stacey%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22S.%20M.%22%2C%22lastName%22%3A%22Kinsella%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22P.%22%2C%22lastName%22%3A%22Sharpe%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22P.%22%2C%22lastName%22%3A%22Phillips%22%7D%5D%2C%22abstractNote%22%3A%22To%20avoid%20potentially%20fatal%20wrong-route%20neuraxial%20drug%20errors%2C%20international%20standard%20ISO%2080369-6%20specifying%20a%20non-Luer%20neuraxial%20connector%20design%20was%20published%20in%202016.%20We%20describe%20usability%20studies%20used%20in%20development%20of%20the%20design.%20Thirty-eight%20doctors%20and%2017%20nurses%20performed%20simulated%20procedures%20on%20manikins%2C%20using%20devices%20fitted%20with%20Luer%20connectors%20or%20draft%20ISO%2080369-6%20%5Cu2018non-Luer%5Cu2019%20connectors.%20The%20procedures%20included%20spinal%20anaesthesia%3B%20intrathecal%20chemotherapy%3B%20lumbar%20puncture%2C%20cerebrospinal%20fluid%20collection%20and%20pressure%20measurement%3B%20epidural%20catheter%20placement%20with%20bolus%20injection%20and%20critical%20care%20use.%20Participants%20attempted%20cross%20connection%20between%20neuraxial%20connectors%20and%20a%20range%20of%20other%20medical%20device%20connectors%2C%20including%20those%20from%20the%20ISO%2080369%20small-bore%20connector%20series.%20Video%20recording%20analysis%20was%20used%20for%20all%20assessments.%20Participants%20subjectively%20assessed%20performance%20of%20the%20draft%20non-Luer%20connector%2C%20including%20suitability%20for%20routine%20clinical%20use.%20Participants%20performed%20198%20procedures.%20The%20connector%20achieved%20easy%2C%20leak-free%20connections.%20The%20willingness%20of%20participants%20to%20use%20the%20non-Luer%20connectors%20were%3A%20spinal%20anaesthesia%20100%25%3B%20intrathecal%20chemotherapy%2088%25%3B%20lumbar%20puncture%2C%20cerebrospinal%20fluid%20collection%20and%20pressure%20measurement%2093%25%3B%20epidural%20catheter%20placement%20with%20bolus%20injection%2078%25%3B%20critical%20care%20use%20100%25.%20Concerns%20raised%20were%20generally%20device%20related%2C%20rather%20than%20connector%20related.%20Most%20cross-connection%20attempts%20failed%2C%20even%20using%20above%20clinical%20forces%20and%2C%20when%20successful%2C%20were%20judged%20of%20low%20clinical%20risk%20potential%3B%20the%20exception%20was%20a%20malaligned%20connection%20between%20the%20non-Luer%20slip%20and%20female%20Luer%20connectors.%20This%20led%20to%20revision%20of%20the%20dimensional%20tolerances%20of%20the%20non-Luer%20connector%20to%20reduce%20this%20risk%2C%20before%20publication%20of%20the%20final%20specification%20in%202016.%20We%20conclude%20that%20the%20ISO%2080369-6%20neuraxial%20non-Luer%20connector%20is%20suitable%20for%20clinical%20use.%22%2C%22date%22%3A%222019%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1111%5C%2Fanae.14585%22%2C%22ISSN%22%3A%221365-2044%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fonlinelibrary.wiley.com%5C%2Fdoi%5C%2Fabs%5C%2F10.1111%5C%2Fanae.14585%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222020-02-16T12%3A07%3A59Z%22%7D%7D%2C%7B%22key%22%3A%22RDEV8DC7%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Cassidy%20et%20al.%22%2C%22parsedDate%22%3A%222011%22%2C%22numChildren%22%3A2%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BCassidy%2C%20C.%20J.%2C%20Smith%2C%20A.%20%26amp%3B%20Arnot%26%23x2010%3BSmith%2C%20J.%20Critical%20incident%20reports%20concerning%20anaesthetic%20equipment%3A%20analysis%20of%20the%20UK%20National%20Reporting%20and%20Learning%20System%20%28NRLS%29%20data%20from%202006%26%23x2013%3B2008%2A.%20%26lt%3Bi%26gt%3BAnaesthesia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B66%26lt%3B%5C%2Fb%26gt%3B%2C%20879%26%23x2013%3B888%20%282011%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Critical%20incident%20reports%20concerning%20anaesthetic%20equipment%3A%20analysis%20of%20the%20UK%20National%20Reporting%20and%20Learning%20System%20%28NRLS%29%20data%20from%202006%5Cu20132008%2A%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22C.%20J.%22%2C%22lastName%22%3A%22Cassidy%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A.%22%2C%22lastName%22%3A%22Smith%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22J.%22%2C%22lastName%22%3A%22Arnot%5Cu2010Smith%22%7D%5D%2C%22abstractNote%22%3A%22Anaesthetic%20equipment%20plays%20a%20central%20role%20in%20anaesthetic%20practice%20but%20brings%20the%20potential%20for%20malfunction%20or%20misuse.%20We%20aimed%20to%20explore%20the%20national%20picture%20by%20reviewing%20patient%20safety%20incidents%20relating%20to%20anaesthetic%20equipment%20from%20the%20National%20Reporting%20and%20Learning%20System%20for%20England%20and%20Wales%20between%202006%20and%202008.%20We%20searched%20the%20database%20using%20the%20system%5Cu2019s%20own%20classification%20and%20by%20scrutinising%20the%20free%20text%20of%20relevant%20incidents.%20There%20were%201029%20relevant%20incidents.%20Of%20these%2C%20410%20%2839.8%25%29%20concerned%20patient%20monitoring%2C%20most%20commonly%20screen%20failure%20during%20anaesthesia%2C%20failure%20of%20one%20modality%20or%20failure%20to%20transfer%20data%20automatically%20from%20anaesthetic%20room%20to%20operating%20theatre.%20Problems%20relating%20to%20ventilators%20made%20up%20185%20%2817.9%25%29%20of%20the%20reports.%20Sudden%20failures%20during%20anaesthesia%20accounted%20for%20142%20%2813.8%25%29%20of%20these%2C%20with%20a%20further%2010%20cases%20%280.9%25%29%20where%20malfunction%20caused%20a%20sustained%20or%20increasing%20positive%20pressure%20in%20the%20patient%5Cu2019s%20airway.%20Leaks%20made%20up%2099%20%289.6%25%29%20of%20incidents%20and%2053%20%285.2%25%29%20of%20incidents%20arose%20from%20the%20use%20of%20infusion%20pumps.%20Most%20%2889%25%29%20of%20the%20incidents%20caused%20no%20patient%20harm%3B%20only%2030%20%282.9%25%29%20were%20judged%20to%20have%20led%20to%20moderate%20or%20severe%20harm.%20Although%20equipment%20was%20often%20faulty%2C%20user%20error%20or%20unfamiliarity%20also%20played%20a%20part.%20A%20large%20variety%20of%20causes%20led%20to%20a%20relatively%20small%20number%20of%20clinical%20scenarios%2C%20that%20anaesthetists%20should%20be%20ready%2C%20both%20individually%20and%20organisationally%2C%20to%20manage%20even%20when%20the%20cause%20is%20not%20apparent.%20We%20make%20recommendations%20for%20enhancing%20patient%20safety%20with%20respect%20to%20equipment.%20You%20can%20respond%20to%20this%20article%20at%20http%3A%5C%2F%5C%2Fwww.anaesthesiacorrespondence.com%22%2C%22date%22%3A%222011%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1111%5C%2Fj.1365-2044.2011.06826.x%22%2C%22ISSN%22%3A%221365-2044%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fonlinelibrary.wiley.com%5C%2Fdoi%5C%2Fabs%5C%2F10.1111%5C%2Fj.1365-2044.2011.06826.x%22%2C%22collections%22%3A%5B%22HF2N89AI%22%5D%2C%22dateModified%22%3A%222020-02-16T12%3A05%3A48Z%22%7D%7D%2C%7B%22key%22%3A%22SB3BQIBY%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22numChildren%22%3A0%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BChecklist%20for%20anaesthetic%20equipment.%202.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Checklist%20for%20anaesthetic%20equipment%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22%22%2C%22language%22%3A%22%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22HF2N89AI%22%5D%2C%22dateModified%22%3A%222020-02-16T12%3A00%3A15Z%22%7D%7D%2C%7B%22key%22%3A%22HFUMC5Y6%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Chair%20et%20al.%22%2C%22parsedDate%22%3A%222009-09-01%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BChair%20%26lt%3Bi%26gt%3Bet%20al.%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bi%26gt%3BSafe%20management%20of%20anaesthetic%20related%20equipment%26lt%3B%5C%2Fi%26gt%3B.%20%26lt%3Ba%20class%3D%26%23039%3Bzp-ItemURL%26%23039%3B%20href%3D%26%23039%3Bhttps%3A%5C%2F%5C%2Fwww.anaesthetists.org%5C%2FHome%5C%2FResources-publications%5C%2FGuidelines%5C%2FSafe-management-of-anaesthetic-related-equipment%26%23039%3B%26gt%3Bhttps%3A%5C%2F%5C%2Fwww.anaesthetists.org%5C%2FHome%5C%2FResources-publications%5C%2FGuidelines%5C%2FSafe-management-of-anaesthetic-related-equipment%26lt%3B%5C%2Fa%26gt%3B%20%282009%29%20doi%3A10.21466%5C%2Fg.SMOAREA.2009.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22report%22%2C%22title%22%3A%22Safe%20management%20of%20anaesthetic%20related%20equipment%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Chair%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Dr%20J%20A%22%2C%22lastName%22%3A%22Carter%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Dr%20L%20W%22%2C%22lastName%22%3A%22Gemmell%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22AAGBI%20Honorary%20Secretary%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Prof%20M%20Y%20K%22%2C%22lastName%22%3A%22Wee%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22AAGBI%20Council%20Member%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Dr%20C%22%2C%22lastName%22%3A%22Meadows%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Immediate%20Past%20GAT%20Chair%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Dr%20T%22%2C%22lastName%22%3A%22Clutton-Brock%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Royal%20College%20of%20Anaesthetists%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Dr%20C%22%2C%22lastName%22%3A%22Waldmann%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Intensive%20Care%20Society%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Dr%20D%22%2C%22lastName%22%3A%22Scott%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22AAGBI%20Standards%20Committee%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Dr%20P%22%2C%22lastName%22%3A%22Bickford-Smith%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22AAGBI%20Standards%20Committee%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Dr%20A%22%2C%22lastName%22%3A%22Wilkes%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Medical%20Device%20Evaluation%20Centre%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Mr%20C%22%2C%22lastName%22%3A%22Bray%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Medicines%20and%20Heathcare%20products%20%20Regulatory%20Agency%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Mr%20D%22%2C%22lastName%22%3A%22McIvor%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Medicines%20and%20Heathcare%20products%20%20Regulatory%20Agency%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Mr%20H%22%2C%22lastName%22%3A%22Cooke%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Barema%2C%20Trade%20Association%20for%20%20Anaesthetic%20%26%20Respiratory%20Equipment%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22reportNumber%22%3A%22%22%2C%22reportType%22%3A%22%22%2C%22institution%22%3A%22The%20Association%20of%20Anaesthetists%20of%20Great%20Britain%20and%20Ireland%22%2C%22date%22%3A%222009-09-01%22%2C%22language%22%3A%22en%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.anaesthetists.org%5C%2FHome%5C%2FResources-publications%5C%2FGuidelines%5C%2FSafe-management-of-anaesthetic-related-equipment%22%2C%22collections%22%3A%5B%22HF2N89AI%22%5D%2C%22dateModified%22%3A%222020-02-16T11%3A56%3A04Z%22%7D%7D%2C%7B%22key%22%3A%22IFUGCDCI%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Association%20of%20Anaesthetists%20of%20Great%20Britain%20and%2C%20Ireland%20et%20al.%22%2C%22parsedDate%22%3A%222012%22%2C%22numChildren%22%3A3%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BAssociation%20of%20Anaesthetists%20of%20Great%20Britain%20and%2C%20Ireland%20%26lt%3Bi%26gt%3Bet%20al.%26lt%3B%5C%2Fi%26gt%3B%20Checking%20Anaesthetic%20Equipment%202012%3A%20Association%20of%20Anaesthetists%20of%20Great%20Britain%20and%20Ireland.%20%26lt%3Bi%26gt%3BAnaesthesia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B67%26lt%3B%5C%2Fb%26gt%3B%2C%20660%26%23x2013%3B668%20%282012%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Checking%20Anaesthetic%20Equipment%202012%3A%20Association%20of%20Anaesthetists%20of%20Great%20Britain%20and%20Ireland%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Association%20of%20Anaesthetists%20of%20Great%20Britain%20and%2C%20Ireland%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22E.%22%2C%22lastName%22%3A%22Anderson%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22V.%22%2C%22lastName%22%3A%22Bythell%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22L.%22%2C%22lastName%22%3A%22Gemmell%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22H.%22%2C%22lastName%22%3A%22Jones%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22D.%22%2C%22lastName%22%3A%22McIvor%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A.%22%2C%22lastName%22%3A%22Pattinson%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22P.%22%2C%22lastName%22%3A%22Sim%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22I.%22%2C%22lastName%22%3A%22Walker%22%7D%5D%2C%22abstractNote%22%3A%22A%20pre-use%20check%20to%20ensure%20the%20correct%20functioning%20of%20anaesthetic%20equipment%20is%20essential%20to%20patient%20safety.%20The%20anaesthetist%20has%20a%20primary%20responsibility%20to%20understand%20the%20function%20of%20the%20anaesthetic%20equipment%20and%20to%20check%20it%20before%20use.%20Anaesthetists%20must%20not%20use%20equipment%20unless%20they%20have%20been%20trained%20to%20use%20it%20and%20are%20competent%20to%20do%20so.%20A%20self-in%5Cufb02ating%20bag%20must%20be%20immediately%20available%20in%20any%20location%20where%20anaesthesia%20may%20be%20given.%20A%20two-bag%20test%20should%20be%20performed%20after%20the%20breathing%20system%2C%20vaporisers%20and%20ventilator%20have%20been%20checked%20individually.%20A%20record%20should%20be%20kept%20with%20the%20anaesthetic%20machine%20that%20these%20checks%20have%20been%20done.%20The%20%5Cu2018%5Cufb01rst%20user%5Cu2019%20check%20after%20servicing%20is%20especially%20important%20and%20must%20be%20recorded.%22%2C%22date%22%3A%2206%5C%2F2012%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1111%5C%2Fj.1365-2044.2012.07163.x%22%2C%22ISSN%22%3A%2200032409%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fdoi.wiley.com%5C%2F10.1111%5C%2Fj.1365-2044.2012.07163.x%22%2C%22collections%22%3A%5B%22HF2N89AI%22%5D%2C%22dateModified%22%3A%222020-02-16T11%3A43%3A21Z%22%7D%7D%2C%7B%22key%22%3A%22T3TYUZCT%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Bourgain%20et%20al.%22%2C%22parsedDate%22%3A%222014%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BBourgain%2C%20J.%20L.%2C%20Coisel%2C%20Y.%2C%20Kern%2C%20D.%2C%20Nouette-Gaulain%2C%20K.%20%26amp%3B%20Panczer%2C%20M.%20What%20are%20the%20main%20%26%23x201C%3Bmachine%20dysfunctions%26%23x201D%3B%20to%20know%3F%20%26lt%3Bi%26gt%3BAnnales%20Fran%26%23xE7%3Baises%20d%26%23x2019%3BAnesth%26%23xE9%3Bsie%20et%20de%20R%26%23xE9%3Banimation%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B33%26lt%3B%5C%2Fb%26gt%3B%2C%20466%26%23x2013%3B471%20%282014%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22What%20are%20the%20main%20%5Cu201cmachine%20dysfunctions%5Cu201d%20to%20know%3F%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22J.L.%22%2C%22lastName%22%3A%22Bourgain%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Y.%22%2C%22lastName%22%3A%22Coisel%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22D.%22%2C%22lastName%22%3A%22Kern%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22K.%22%2C%22lastName%22%3A%22Nouette-Gaulain%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22M.%22%2C%22lastName%22%3A%22Panczer%22%7D%5D%2C%22abstractNote%22%3A%22The%20incidents%20related%20to%20the%20medical%20devices%20are%20common%20during%20anesthesia%20and%20in%20intensive%20care%20unit.%20These%20incidents%20are%20rarely%20the%20cause%20of%20complications%20because%20monitoring%20detects%20them%20early%3B%20alternative%20scenarios%20allow%20bearing%20these%20problems.%20Although%20the%20incidence%20of%20these%20complications%20has%20much%20declined%2C%20these%20incidents%20are%20serious%20adverse%20events%20and%20at%20the%20origin%20of%20life-threatening%20complications.%20Improper%20use%20of%20medical%20devices%20is%20the%20main%20factor%20that%20promotes%20the%20onset%20of%20these%20complications.%20To%20maintain%20a%20high%20level%20of%20security%2C%20it%20is%20necessary%20to%20use%20and%20control%20procedures%20according%20to%20the%20manufacturer%20recommendations.%20This%20is%20part%20of%20a%20strategy%20involving%20users%2C%20biomedical%20engineers%20and%20manufacturers.%20Several%20actions%20are%20effective%20in%20preventing%20the%20occurrence%20of%20these%20incidents%3A%20the%20control%20before%20use%2C%20the%20continuation%20of%20the%20performance%20of%20the%20equipment%2C%20use%20based%20on%20the%20recommendations%20of%20the%20experts%20and%20manufacturers%20and%20appropriate%20training.%20This%20strategy%20is%20best%20applied%20by%20a%20clinical%20expert%20who%20has%20extensive%20technical%20knowledge.%20This%20expert%20is%20a%20key%20player%20for%20users%20learning%20and%20allows%20establishing%20and%20maintaining%20rules%20of%20use%20in%20collaboration%20with%20medical%20staff%20and%20biomedical%20engineers%20and%20manufacturers.%22%2C%22date%22%3A%2207%5C%2F2014%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.annfar.2014.07.744%22%2C%22ISSN%22%3A%2207507658%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Flinkinghub.elsevier.com%5C%2Fretrieve%5C%2Fpii%5C%2FS0750765814009940%22%2C%22collections%22%3A%5B%22HF2N89AI%22%5D%2C%22dateModified%22%3A%222020-02-16T10%3A59%3A37Z%22%7D%7D%2C%7B%22key%22%3A%22IUTP39SR%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Orihara%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BOrihara%2C%20M.%20Comparison%20of%20incidence%20of%20anaphylaxis%20between%20sugammadex%20and%20neostigmine%3A%20a%20retrospective%20multicentre%20observational%20study.%2010.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Comparison%20of%20incidence%20of%20anaphylaxis%20between%20sugammadex%20and%20neostigmine%3A%20a%20retrospective%20multicentre%20observational%20study%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Masaki%22%2C%22lastName%22%3A%22Orihara%22%7D%5D%2C%22abstractNote%22%3A%22Background%3A%20Although%20cases%20of%20anaphylaxis%20caused%20by%20sugammadex%20have%20been%20reported%2C%20its%20incidence%20remains%20uncertain.%20Conversely%2C%20no%20studies%20have%20evaluated%20the%20incidence%20of%20anaphylaxis%20to%20neostigmine.%5CnMethods%3A%20This%20was%20a%20retrospective%20multicentre%20observational%20study%20of%20patients%20who%20underwent%20surgery%20under%20general%20anaesthesia%20between%202012%20and%202016%20to%20compare%20the%20incidence%20of%20anaphylaxis%20with%20sugammadex%20with%20that%20of%20neostigmine%20at%20four%20tertiary%20hospitals%20in%20Japan.%20To%20ensure%20the%20quality%20of%20diagnosis%2C%20only%20cases%20with%20a%20clinical%20history%20suggestive%20of%20anaphylaxis%2C%20along%20with%20positive%20results%20from%20in%20vitro%20or%20in%20vivo%20testing%2C%20were%20assessed.%5CnResults%3A%20From%20a%20total%20of%2049%20532%20patients%20who%20received%20general%20anaesthesia%20included%20in%20this%20study%2C%2018%20cases%20of%20anaphylaxis%20were%20reported%2C%20of%20which%20six%20were%20attributable%20to%20sugammadex%20and%20none%20to%20neostigmine.%20There%20were%20no%20fatalities%20attributable%20to%20anaphylaxis.%20The%20incidence%20of%20anaphylaxis%20caused%20by%20all%20drugs%20or%20by%20sugammadex%20was%20calculated%20as%200.036%25%20%2895%25%20con%5Cufb01dence%20interval%20%5BCI%5D%3A%200.022e0.057%25%29%20and%200.02%25%20%28of%20the%20number%20of%20sugammadex%20cases%29%20%2895%25%20CI%3A%200.007e0.044%25%29%2C%20respectively.%5CnConclusions%3A%20The%20results%20suggest%20that%20neostigmine%20might%20be%20safer%20than%20sugammadex%20when%20assessing%20only%20the%20incidence%20of%20anaphylaxis.%20We%20believe%20that%20there%20is%20room%20for%20reconsideration%20of%20the%20choice%20of%20reversal%20agent%20for%20neuromuscular%20blocking%20agents%20by%20all%20anaesthetists.%20Clinical%20trial%20registration%3A%20UMIN000022365%3B%20UMIN000033561.%22%2C%22date%22%3A%22%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-12-02T03%3A26%3A56Z%22%7D%7D%2C%7B%22key%22%3A%22B3QKMVTM%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Xie%20and%20Carayon%22%2C%22parsedDate%22%3A%222015-01-02%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BXie%2C%20A.%20%26amp%3B%20Carayon%2C%20P.%20A%20systematic%20review%20of%20human%20factors%20and%20ergonomics%20%28HFE%29-based%20healthcare%20system%20redesign%20for%20quality%20of%20care%20and%20patient%20safety.%20%26lt%3Bi%26gt%3BErgonomics%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B58%26lt%3B%5C%2Fb%26gt%3B%2C%2033%26%23x2013%3B49%20%282015%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22A%20systematic%20review%20of%20human%20factors%20and%20ergonomics%20%28HFE%29-based%20healthcare%20system%20redesign%20for%20quality%20of%20care%20and%20patient%20safety%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Anping%22%2C%22lastName%22%3A%22Xie%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Pascale%22%2C%22lastName%22%3A%22Carayon%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222015-01-02%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1080%5C%2F00140139.2014.959070%22%2C%22ISSN%22%3A%220014-0139%2C%201366-5847%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fwww.tandfonline.com%5C%2Fdoi%5C%2Fabs%5C%2F10.1080%5C%2F00140139.2014.959070%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A51%3A13Z%22%7D%7D%2C%7B%22key%22%3A%22XBHK2FX4%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Wilkes%22%2C%22parsedDate%22%3A%222002%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BWilkes%2C%20A.%20R.%20Measuring%20the%20filtration%20performance%20of%20breathing%20system%20filters%20using%20sodium%20chloride%20particles.%207%20%282002%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Measuring%20the%20filtration%20performance%20of%20breathing%20system%20filters%20using%20sodium%20chloride%20particles%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A%20R%22%2C%22lastName%22%3A%22Wilkes%22%7D%5D%2C%22abstractNote%22%3A%22The%20filtration%20performance%20of%2033%20breathing%20system%20filters%20%28nine%20pleated%20hydrophobic%20and%2024%20electrostatic%20filters%29%20was%20measured%20using%20sodium%20chloride%20particles.%20The%20particles%20had%20a%20size%20distribution%20with%20a%20count%20median%20diameter%20of%200.07%20mm%20and%20a%20geometric%20standard%20deviation%20not%20exceeding%201.83.%20The%20geometric%20mean%20penetration%20values%20ranged%20from%200.002%20to%200.67%25%20for%20the%20nine%20pleated%20hydrophobic%20filters%20and%20from%200.25%20to%2035%25%20for%20the%2024%20electrostatic%20filters%20%28p%20%2C%200.0001%20for%20the%20difference%20between%20the%20two%20filter%20types%29.%20The%20filtration%20performance%20obtained%20when%20filters%20are%20challenged%20with%20either%20sodium%20chloride%20particles%20or%20microbes%20is%20compared%20and%20discussed.%22%2C%22date%22%3A%222002%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22X8ZVJS4A%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A50%3A44Z%22%7D%7D%2C%7B%22key%22%3A%22WQKCYHAQ%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Merry%20et%20al.%22%2C%22parsedDate%22%3A%222011%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BMerry%2C%20A.%20F.%2C%20Shipp%2C%20D.%20H.%20%26amp%3B%20Lowinger%2C%20J.%20S.%20The%20contribution%20of%20labelling%20to%20safe%20medication%20administration%20in%20anaesthetic%20practice.%20%26lt%3Bi%26gt%3BBest%20Practice%20%26amp%3B%20Research%20Clinical%20Anaesthesiology%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B25%26lt%3B%5C%2Fb%26gt%3B%2C%20145%26%23x2013%3B159%20%282011%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22The%20contribution%20of%20labelling%20to%20safe%20medication%20administration%20in%20anaesthetic%20practice%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Alan%20F.%22%2C%22lastName%22%3A%22Merry%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Diana%20H.%22%2C%22lastName%22%3A%22Shipp%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jocelyn%20S.%22%2C%22lastName%22%3A%22Lowinger%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%226%5C%2F2011%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.bpa.2011.02.009%22%2C%22ISSN%22%3A%2215216896%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Flinkinghub.elsevier.com%5C%2Fretrieve%5C%2Fpii%5C%2FS1521689611000280%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A48%3A50Z%22%7D%7D%2C%7B%22key%22%3A%222EP9MZMW%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Shultz%20et%20al.%22%2C%22parsedDate%22%3A%222010%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BShultz%2C%20J.%20%26lt%3Bi%26gt%3Bet%20al.%26lt%3B%5C%2Fi%26gt%3B%20Standardizing%20anesthesia%20medication%20drawers%20using%20human%20factors%20and%20quality%20assurance%20methods.%20%26lt%3Bi%26gt%3BCanadian%20Journal%20of%20Anesthesia%5C%2FJournal%20canadien%20d%26%23x2019%3Banesth%26%23xE9%3Bsie%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B57%26lt%3B%5C%2Fb%26gt%3B%2C%20490%26%23x2013%3B499%20%282010%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Standardizing%20anesthesia%20medication%20drawers%20using%20human%20factors%20and%20quality%20assurance%20methods%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jonas%22%2C%22lastName%22%3A%22Shultz%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jan%20M.%22%2C%22lastName%22%3A%22Davies%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jeff%22%2C%22lastName%22%3A%22Caird%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Susan%22%2C%22lastName%22%3A%22Chisholm%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Karen%22%2C%22lastName%22%3A%22Ruggles%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Raymond%22%2C%22lastName%22%3A%22Puls%22%7D%5D%2C%22abstractNote%22%3A%22Purpose%20In%20Calgary%2C%20each%20of%20the%20three%20acute-care%20adult%20hospitals%20had%20different%20anesthetic%20medication%20carts%20with%20their%20own%20type%20and%20layout%20of%20anesthetic%20medications.%20A%20number%20of%20anesthesiologists%20moved%20among%20the%20different%20sites%2C%20increasing%20the%20potential%20for%20medication%20errors.%20The%20objective%20of%20this%20study%20was%20to%20identify%20the%20anesthetic%20medications%20to%20include%20and%20to%20determine%20how%20they%20should%20be%20grouped%20and%20positioned%20in%20a%20standardized%20anesthesia%20medication%20cart%20drawer.%22%2C%22date%22%3A%225%5C%2F2010%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1007%5C%2Fs12630-010-9274-8%22%2C%22ISSN%22%3A%220832-610X%2C%201496-8975%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Flink.springer.com%5C%2F10.1007%5C%2Fs12630-010-9274-8%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A45%3A43Z%22%7D%7D%2C%7B%22key%22%3A%22VLM4FM34%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Holloway%20and%20Johnson%22%2C%22parsedDate%22%3A%222011%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BHolloway%2C%20C.%20M.%20%26amp%3B%20Johnson%2C%20C.%20W.%20Reducing%20our%20ignorance%3A%20finding%20answers%20to%20certain%20epistemic%20questions%20for%20software%20systems.%20in%20%26lt%3Bi%26gt%3B6th%20IET%20International%20Conference%20on%20System%20Safety%202011%26lt%3B%5C%2Fi%26gt%3B%20D12%26%23x2013%3BD12%20%28IET%2C%202011%29.%20%26lt%3Ba%20class%3D%26%23039%3Bzp-DOIURL%26%23039%3B%20href%3D%26%23039%3Bhttp%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1049%5C%2Fcp.2011.0269%26%23039%3B%26gt%3Bhttp%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1049%5C%2Fcp.2011.0269%26lt%3B%5C%2Fa%26gt%3B.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22conferencePaper%22%2C%22title%22%3A%22Reducing%20our%20ignorance%3A%20finding%20answers%20to%20certain%20epistemic%20questions%20for%20software%20systems%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22C.M.%22%2C%22lastName%22%3A%22Holloway%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22C.W.%22%2C%22lastName%22%3A%22Johnson%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222011%22%2C%22proceedingsTitle%22%3A%226th%20IET%20International%20Conference%20on%20System%20Safety%202011%22%2C%22conferenceName%22%3A%226th%20IET%20International%20Conference%20on%20System%20Safety%202011%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1049%5C%2Fcp.2011.0269%22%2C%22ISBN%22%3A%22978-1-84919-535-5%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fdigital-library.theiet.org%5C%2Fcontent%5C%2Fconferences%5C%2F10.1049%5C%2Fcp.2011.0269%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A43%3A21Z%22%7D%7D%2C%7B%22key%22%3A%22QD4MSCJG%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Arthmar%22%2C%22parsedDate%22%3A%222015%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BArthmar%2C%20R.%20VILFREDO%20PARETO.%20Manual%20of%20Political%20Economy.%20A%20critical%20and%20variorum%20edition.%20Edited%20by%20Aldo%20Montesano%2C%20Alberto%20Zanni%2C%20Luigino%20Bruni%2C%20John%20Chipman%20and%20Michael%20McLure.%20Oxford%3A%20Oxford%20University%20Press%2C%202014%2C%20664%20p.%20%26lt%3Bi%26gt%3BEstudos%20Econ%26%23xF4%3Bmicos%20%28S%26%23xE3%3Bo%20Paulo%29%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B45%26lt%3B%5C%2Fb%26gt%3B%2C%20459%26%23x2013%3B470%20%282015%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22VILFREDO%20PARETO.%20Manual%20of%20Political%20Economy.%20A%20critical%20and%20variorum%20edition.%20Edited%20by%20Aldo%20Montesano%2C%20Alberto%20Zanni%2C%20Luigino%20Bruni%2C%20John%20Chipman%20and%20Michael%20McLure.%20Oxford%3A%20Oxford%20University%20Press%2C%202014%2C%20664%20p.%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Rog%5Cu00e9rio%22%2C%22lastName%22%3A%22Arthmar%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2206%5C%2F2015%22%2C%22language%22%3A%22pt%22%2C%22DOI%22%3A%2210.1590%5C%2F0101-4161201545258roa%22%2C%22ISSN%22%3A%220101-4161%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fwww.scielo.br%5C%2Fscielo.php%3Fscript%3Dsci_arttext%26pid%3DS0101-41612015000200459%26lng%3Dpt%26tlng%3Dpt%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A37%3A31Z%22%7D%7D%2C%7B%22key%22%3A%22SFU3URUS%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Donzelli%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BDonzelli%2C%20F.%20Pareto%26%23x2019%3Bs%20Mechanical%20Dream.%2047.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Pareto%27s%20Mechanical%20Dream%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Franco%22%2C%22lastName%22%3A%22Donzelli%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A36%3A58Z%22%7D%7D%2C%7B%22key%22%3A%22B3H7G93A%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Muschara%22%2C%22parsedDate%22%3A%222014%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BMuschara%2C%20T.%20Critical%20Steps%3A%20How%20to%20Identify%20and%20Manage%20the%20Most%20Important%20Human%20Performance%20Risks%20in%20Operations.%20%26lt%3Bi%26gt%3BPerformance%20Improvement%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B53%26lt%3B%5C%2Fb%26gt%3B%2C%2011%26%23x2013%3B21%20%282014%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Critical%20Steps%3A%20How%20to%20Identify%20and%20Manage%20the%20Most%20Important%20Human%20Performance%20Risks%20in%20Operations%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Tony%22%2C%22lastName%22%3A%22Muschara%22%7D%5D%2C%22abstractNote%22%3A%22A%20critical%20step%20is%20defined%20as%20a%20human%20action%20that%20will%20trigger%20immediate%2C%20irreversible%2C%20and%20intolerable%20harm%20to%20an%20asset%2C%20if%20that%20action%20or%20a%20preceding%20action%20is%20performed%20improperly.%20Critical%20steps%20occur%20anytime%20an%20action%20involves%20a%20substantial%20transfer%20of%20energy%2C%20the%20movement%20of%20mass%2C%20or%20the%20transmission%20of%20information%20that%2C%20if%20not%20performed%20under%20control%2C%20could%20result%20in%20serious%20harm%20to%20an%20organization%5Cu2019s%20assets.%20Accidents%20typically%20occur%20when%20front%20line%20production%20personnel%20lose%20control%20of%20such%20transfers%20during%20work.%20Human%20beings%2C%20because%20of%20human%20fallibility%2C%20are%20the%20greatest%20source%20of%20variation%20in%20operations.%20First%2C%20this%20paper%20describes%20the%20critical%20step%20concept%20and%20the%20preceding%20conditions%5Cu2014risk-important%20actions%5Cu2014that%20create%20critical%20steps.%20Second%2C%20a%20couple%20of%20means%20of%20managing%20and%20controlling%20performance%20of%20critical%20steps%20during%20operations%20are%20described.%20Included%20is%20an%20adaptation%20of%20the%20cornerstones%20of%20resilience%20described%20by%20Erik%20Hollnagel%20in%20the%20Ashgate%20series%20on%20Resilience%20Engineering.%20Risk-based%20thinking%5Cu2014anticipate%2C%20monitor%2C%20respond%2C%20and%20learn%5Cu2014is%20offered%20as%20a%20fundamental%20first%20principal%20of%20identifying%20and%20controlling%20the%20performance%20of%20critical%20steps%20during%20operations.%22%2C%22date%22%3A%2210%5C%2F2014%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1002%5C%2Fpfi.21437%22%2C%22ISSN%22%3A%2210908811%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fdoi.wiley.com%5C%2F10.1002%5C%2Fpfi.21437%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A31%3A36Z%22%7D%7D%2C%7B%22key%22%3A%2245SN7Q26%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Keijzer%20et%20al.%22%2C%22parsedDate%22%3A%222007%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BKeijzer%2C%20C.%2C%20Perez%2C%20R.%20S.%20G.%20M.%20%26amp%3B%20de%20Lange%2C%20J.%20J.%20Compound%20A%20and%20carbon%20monoxide%20production%20from%20sevoflurane%20and%20seven%20different%20types%20of%20carbon%20dioxide%20absorbent%20in%20a%20patient%20model.%20%26lt%3Bi%26gt%3BActa%20Anaesthesiologica%20Scandinavica%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B51%26lt%3B%5C%2Fb%26gt%3B%2C%2031%26%23x2013%3B37%20%282007%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Compound%20A%20and%20carbon%20monoxide%20production%20from%20sevoflurane%20and%20seven%20different%20types%20of%20carbon%20dioxide%20absorbent%20in%20a%20patient%20model%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22C.%22%2C%22lastName%22%3A%22Keijzer%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22R.%20S.%20G.%20M.%22%2C%22lastName%22%3A%22Perez%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22J.%20J.%22%2C%22lastName%22%3A%22de%20Lange%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2201%5C%2F2007%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1111%5C%2Fj.1399-6576.2006.01187.x%22%2C%22ISSN%22%3A%220001-5172%2C%201399-6576%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fdoi.wiley.com%5C%2F10.1111%5C%2Fj.1399-6576.2006.01187.x%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A29%3A26Z%22%7D%7D%2C%7B%22key%22%3A%22TVC7AI4W%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Saito%22%2C%22parsedDate%22%3A%222013%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BSaito%2C%20M.%20Brown%20Adipose%20Tissue%20as%20a%20Regulator%20of%20Energy%20Expenditure%20and%20Body%20Fat%20in%20Humans.%20%26lt%3Bi%26gt%3BDiabetes%20%26amp%3B%20Metabolism%20Journal%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B37%26lt%3B%5C%2Fb%26gt%3B%2C%2022%20%282013%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Brown%20Adipose%20Tissue%20as%20a%20Regulator%20of%20Energy%20Expenditure%20and%20Body%20Fat%20in%20Humans%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Masayuki%22%2C%22lastName%22%3A%22Saito%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222013%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.4093%5C%2Fdmj.2013.37.1.22%22%2C%22ISSN%22%3A%222233-6079%2C%202233-6087%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fsynapse.koreamed.org%5C%2FDOIx.php%3Fid%3D10.4093%5C%2Fdmj.2013.37.1.22%22%2C%22collections%22%3A%5B%22KMIJV538%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A17%3A17Z%22%7D%7D%2C%7B%22key%22%3A%22A8JKTG5M%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Razzouk%20and%20Shute%22%2C%22parsedDate%22%3A%222012%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BRazzouk%2C%20R.%20%26amp%3B%20Shute%2C%20V.%20What%20Is%20Design%20Thinking%20and%20Why%20Is%20It%20Important%3F%20%26lt%3Bi%26gt%3BReview%20of%20Educational%20Research%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B82%26lt%3B%5C%2Fb%26gt%3B%2C%20330%26%23x2013%3B348%20%282012%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22What%20Is%20Design%20Thinking%20and%20Why%20Is%20It%20Important%3F%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Rim%22%2C%22lastName%22%3A%22Razzouk%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Valerie%22%2C%22lastName%22%3A%22Shute%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2209%5C%2F2012%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.3102%5C%2F0034654312457429%22%2C%22ISSN%22%3A%220034-6543%2C%201935-1046%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fjournals.sagepub.com%5C%2Fdoi%5C%2F10.3102%5C%2F0034654312457429%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T11%3A15%3A27Z%22%7D%7D%2C%7B%22key%22%3A%228VTS4AT7%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Lally%20et%20al.%22%2C%22parsedDate%22%3A%222009%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BLally%2C%20P.%2C%20Potts%2C%20H.%20W.%20W.%20%26amp%3B%20Wardle%2C%20J.%20Research%20article%20How%20are%20habits%20formed%3A%20Modelling%20habit%20formation%20in%20the%20real%20worldy.%20%26lt%3Bi%26gt%3BEur.%20J.%20Soc.%20Psychol.%26lt%3B%5C%2Fi%26gt%3B%2013%20%282009%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Research%20article%20How%20are%20habits%20formed%3A%20Modelling%20habit%20formation%20in%20the%20real%20worldy%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Phillippa%22%2C%22lastName%22%3A%22Lally%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Henry%20W%20W%22%2C%22lastName%22%3A%22Potts%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jane%22%2C%22lastName%22%3A%22Wardle%22%7D%5D%2C%22abstractNote%22%3A%22To%20investigate%20the%20process%20of%20habit%20formation%20in%20everyday%20life%2C%2096%20volunteers%20chose%20an%20eating%2C%20drinking%20or%20activity%20behaviour%20to%20carry%20out%20daily%20in%20the%20same%20context%20%28for%20example%20%5Cu2018after%20breakfast%5Cu2019%29%20for%2012%20weeks.%20They%20completed%20the%20self-report%20habit%20index%20%28SRHI%29%20each%20day%20and%20recorded%20whether%20they%20carried%20out%20the%20behaviour.%20The%20majority%20%2882%29%20of%20participants%20provided%20suf%5Cufb01cient%20data%20for%20analysis%2C%20and%20increases%20in%20automaticity%20%28calculated%20with%20a%20sub-set%20of%20SRHI%20items%29%20were%20examined%20over%20the%20study%20period.%20Nonlinear%20regressions%20%5Cufb01tted%20an%20asymptotic%20curve%20to%20each%20individual%5Cu2019s%20automaticity%20scores%20over%20the%2084%20days.%20The%20model%20%5Cufb01tted%20for%2062%20individuals%2C%20of%20whom%2039%20showed%20a%20good%20%5Cufb01t.%20Performing%20the%20behaviour%20more%20consistently%20was%20associated%20with%20better%20model%20%5Cufb01t.%20The%20time%20it%20took%20participants%20to%20reach%2095%25%20of%20their%20asymptote%20of%20automaticity%20ranged%20from%2018%20to%20254%20days%3B%20indicating%20considerable%20variation%20in%20how%20long%20it%20takes%20people%20to%20reach%20their%20limit%20of%20automaticity%20and%20highlighting%20that%20it%20can%20take%20a%20very%20long%20time.%20Missing%20one%20opportunity%20to%20perform%20the%20behaviour%20did%20not%20materially%20affect%20the%20habit%20formation%20process.%20With%20repetition%20of%20a%20behaviour%20in%20a%20consistent%20context%2C%20automaticity%20increases%20following%20an%20asymptotic%20curve%20which%20can%20be%20modelled%20at%20the%20individual%20level.%20Copyright%20%23%202009%20John%20Wiley%20%26amp%3B%20Sons%2C%20Ltd.%22%2C%22date%22%3A%222009%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T07%3A57%3A29Z%22%7D%7D%2C%7B%22key%22%3A%223JHW4DSJ%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Catchpole%20et%20al.%22%2C%22parsedDate%22%3A%222008%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BCatchpole%2C%20K.%2C%20Bell%2C%20M.%20D.%20D.%20%26amp%3B%20Johnson%2C%20S.%20Safety%20in%20anaesthesia%3A%20a%20study%20of%2012%20606%20reported%20incidents%20from%20the%20UK%20National%20Reporting%20and%20Learning%20System.%20%26lt%3Bi%26gt%3BAnaesthesia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B63%26lt%3B%5C%2Fb%26gt%3B%2C%20340%26%23x2013%3B346%20%282008%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Safety%20in%20anaesthesia%3A%20a%20study%20of%2012%20606%20reported%20incidents%20from%20the%20UK%20National%20Reporting%20and%20Learning%20System%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22K.%22%2C%22lastName%22%3A%22Catchpole%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22M.%20D.%20D.%22%2C%22lastName%22%3A%22Bell%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22S.%22%2C%22lastName%22%3A%22Johnson%22%7D%5D%2C%22abstractNote%22%3A%22The%20incident%20reporting%20database%20at%20the%20National%20Patient%20Safety%20Agency%20was%20interrogated%20on%20the%20nature%2C%20frequency%20and%20severity%20of%20incidents%20related%20to%20anaesthesia.%20Of%2012%20606%20reports%20over%20a%202-year%20period%2C%202842%20%2822.5%25%29%20resulted%20in%20little%20harm%20or%20a%20moderate%20degree%20of%20harm%2C%20and%20269%20%282.1%25%29%20resulted%20in%20severe%20harm%20or%20death%2C%20with%20procedure%20or%20treatment%20problems%20generating%20the%20highest%20risk.%20One%20thousand%20and%20thirty-%5Cufb01ve%20incidents%20%288%25%29%20related%20to%20pre-operative%20assessment%2C%20with%20harm%20occurring%20in%20275%20%2826.6%25%29%2C%20and%20552%20%284.4%25%29%20related%20to%20epidural%20anaesthesia%2C%20with%20harm%20reported%20in%20198%20%2835.9%25%29.%20Fifty-eight%20occurrences%20of%20anaesthetic%20awareness%20were%20also%20examined.%20This%20preliminary%20analysis%20is%20not%20authoritative%20enough%20to%20warrant%20widespread%20changes%20of%20practice%2C%20but%20justi%5Cufb01es%20future%20collaborative%20approaches%20to%20reduce%20the%20potential%20for%20harm%20and%20improve%20the%20submission%2C%20collection%20and%20analysis%20of%20incident%20reports.%20Practitioners%2C%20departments%20and%20professional%20bodies%20should%20consider%20how%20the%20information%20can%20be%20used%20to%20promote%20patient%20safety%20and%20their%20own%20defensibility.%22%2C%22date%22%3A%2204%5C%2F2008%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1111%5C%2Fj.1365-2044.2007.05427.x%22%2C%22ISSN%22%3A%220003-2409%2C%201365-2044%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fdoi.wiley.com%5C%2F10.1111%5C%2Fj.1365-2044.2007.05427.x%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T07%3A54%3A25Z%22%7D%7D%2C%7B%22key%22%3A%22QBQMH9KA%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Nedergaard%20et%20al.%22%2C%22parsedDate%22%3A%222007%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BNedergaard%2C%20J.%2C%20Bengtsson%2C%20T.%20%26amp%3B%20Cannon%2C%20B.%20Unexpected%20evidence%20for%20active%20brown%20adipose%20tissue%20in%20adult%20humans.%20%26lt%3Bi%26gt%3BAmerican%20Journal%20of%20Physiology-Endocrinology%20and%20Metabolism%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B293%26lt%3B%5C%2Fb%26gt%3B%2C%20E444%26%23x2013%3BE452%20%282007%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Unexpected%20evidence%20for%20active%20brown%20adipose%20tissue%20in%20adult%20humans%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jan%22%2C%22lastName%22%3A%22Nedergaard%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Tore%22%2C%22lastName%22%3A%22Bengtsson%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Barbara%22%2C%22lastName%22%3A%22Cannon%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2208%5C%2F2007%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1152%5C%2Fajpendo.00691.2006%22%2C%22ISSN%22%3A%220193-1849%2C%201522-1555%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.physiology.org%5C%2Fdoi%5C%2F10.1152%5C%2Fajpendo.00691.2006%22%2C%22collections%22%3A%5B%22KMIJV538%22%5D%2C%22dateModified%22%3A%222019-10-28T07%3A43%3A40Z%22%7D%7D%2C%7B%22key%22%3A%223EPKQ6TK%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Kothari%20and%20Agrawal%22%2C%22parsedDate%22%3A%222013%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BKothari%2C%20D.%20%26amp%3B%20Agrawal%2C%20J.%20Colour-coded%20syringe%20labels%3A%20a%20modification%20to%20enhance%20patient%20safety.%20%26lt%3Bi%26gt%3BBritish%20Journal%20of%20Anaesthesia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B110%26lt%3B%5C%2Fb%26gt%3B%2C%201056%26%23x2013%3B1058%20%282013%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Colour-coded%20syringe%20labels%3A%20a%20modification%20to%20enhance%20patient%20safety%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22D.%22%2C%22lastName%22%3A%22Kothari%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22J.%22%2C%22lastName%22%3A%22Agrawal%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2206%5C%2F2013%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1093%5C%2Fbja%5C%2Faet140%22%2C%22ISSN%22%3A%2200070912%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Flinkinghub.elsevier.com%5C%2Fretrieve%5C%2Fpii%5C%2FS0007091217538751%22%2C%22collections%22%3A%5B%224TK53P7R%22%5D%2C%22dateModified%22%3A%222019-10-28T07%3A42%3A25Z%22%7D%7D%2C%7B%22key%22%3A%22VAKK5ZPC%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Furniss%20et%20al.%22%2C%22parsedDate%22%3A%222019-04-15%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BFurniss%2C%20D.%2C%20Dean%20Franklin%2C%20B.%20%26amp%3B%20Blandford%2C%20A.%20The%20devil%20is%20in%20the%20detail%3A%20How%20a%20closed-loop%20documentation%20system%20for%20IV%20infusion%20administration%20contributes%20to%20and%20compromises%20patient%20safety.%20%26lt%3Bi%26gt%3BHealth%20Informatics%20Journal%26lt%3B%5C%2Fi%26gt%3B%20146045821983957%20%282019%29%20%26lt%3Ba%20class%3D%26%23039%3Bzp-DOIURL%26%23039%3B%20href%3D%26%23039%3Bhttp%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1177%5C%2F1460458219839574%26%23039%3B%26gt%3Bhttp%3A%5C%2F%5C%2Fdoi.org%5C%2F10.1177%5C%2F1460458219839574%26lt%3B%5C%2Fa%26gt%3B.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22The%20devil%20is%20in%20the%20detail%3A%20How%20a%20closed-loop%20documentation%20system%20for%20IV%20infusion%20administration%20contributes%20to%20and%20compromises%20patient%20safety%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Dominic%22%2C%22lastName%22%3A%22Furniss%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Bryony%22%2C%22lastName%22%3A%22Dean%20Franklin%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Ann%22%2C%22lastName%22%3A%22Blandford%22%7D%5D%2C%22abstractNote%22%3A%22Many%20studies%20have%20highlighted%20the%20patient%20safety%20risks%20in%20intravenous%20medication%20administration%2C%20and%20various%20technological%20solutions%20have%20been%20proposed%20to%20mitigate%20those%20risks%2C%20including%20%5Cu2018smart%20pumps%5Cu2019%20and%20closed-loop%20systems.%20Few%20studies%20describe%20these%20implementations%20in%20detail.%20In%20this%20article%2C%20we%20report%20on%20a%20sociotechnical%20investigation%20of%20a%20closed-loop%20documentation%20system%20linked%20with%20smart%20pumps%20for%20intravenous%20infusion%20administration%20on%20an%20intensive%20care%20unit.%20The%20smart%20pumps%20are%20%5Cu2018mapped%5Cu2019%20to%20an%20electronic%20prescribing%20and%20medication%20administration%20system%2C%20allowing%20infusion%20rates%2C%20volumes%20and%20boluses%20of%20intravenous%20medication%20to%20be%20monitored%20in%20real%20time.%20Ethnographic%20observations%20were%20conducted%20over%2037%20h%2C%20including%20direct%20observation%20of%20infusion%20administration%20%28n%5Cu2009%3D%5Cu200923%20infusions%29%2C%20discussions%20with%20clinical%20staff%20and%20semi-structured%20interviews%20with%20intensive%20care%20unit%20managers%20%28n%5Cu2009%3D%5Cu20092%29.%20Analysis%20was%20based%20on%20the%20Distributed%20Cognition%20for%20Teamwork%20%28DiCoT%29%20method%20to%20understand%20how%20information%20is%20processed%20across%20individuals%2C%20teams%20and%20technologies.%20We%20report%20on%20how%20the%20system%20works%20in%20context%2C%20and%20identify%20contributions%20and%20compromises%20to%20patient%20safety%20with%20new%20risks%20that%20need%20to%20be%20managed%20at%20bedside%20and%20intensive%20care%20unit%20level.%22%2C%22date%22%3A%222019-04-15%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1177%5C%2F1460458219839574%22%2C%22ISSN%22%3A%221460-4582%2C%201741-2811%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fjournals.sagepub.com%5C%2Fdoi%5C%2F10.1177%5C%2F1460458219839574%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T07%3A05%3A46Z%22%7D%7D%2C%7B%22key%22%3A%22WFVM2MY6%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Langer%20et%20al.%22%2C%22parsedDate%22%3A%222015-12-29%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BLanger%2C%20T.%20%26lt%3Bi%26gt%3Bet%20al.%26lt%3B%5C%2Fi%26gt%3B%20Intravenous%20balanced%20solutions%3A%20from%20physiology%20to%20clinical%20evidence.%20%26lt%3Bi%26gt%3BAnestezjologia%20Intensywna%20Terapia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B47%26lt%3B%5C%2Fb%26gt%3B%2C%2078%26%23x2013%3B88%20%282015%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Intravenous%20balanced%20solutions%3A%20from%20physiology%20to%20clinical%20evidence%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Thomas%22%2C%22lastName%22%3A%22Langer%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Alessandro%22%2C%22lastName%22%3A%22Santini%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Eleonora%22%2C%22lastName%22%3A%22Scotti%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Niels%22%2C%22lastName%22%3A%22Van%20Regenmortel%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Manu%20L.N.G.%22%2C%22lastName%22%3A%22Malbrain%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Pietro%22%2C%22lastName%22%3A%22Caironi%22%7D%5D%2C%22abstractNote%22%3A%22Balanced%5Cu201d%20solutions%20are%20commonly%20defined%20as%20intravenous%20fluids%20having%20an%20electrolyte%20composition%20close%20to%20that%20of%20plasma.%20As%20such%2C%20they%20should%20minimally%20affect%20acid-base%20equilibrium%2C%20as%20compared%20to%20the%20commonly%20reported%200.9%25%20NaCl-related%20hyperchloremic%20metabolic%20acidosis.%20Recently%2C%20the%20term%20%5Cu201cbalanced%5Cu201d%20solution%20has%20been%20also%20employed%20to%20indicate%20intravenous%20fluids%20with%20low%20chloride%20content%2C%20being%20the%20concentration%20of%20this%20electrolyte%20the%20most%20altered%20in%200.9%25%20NaCl%20as%20compared%20to%20plasma%2C%20and%20based%20upon%20a%20suggested%20detrimental%20alteration%20of%20renal%20function%20associated%20with%20hyperchloremia.%20Despite%20efforts%20made%20towards%20its%20identification%2C%20the%20ideal%20balanced%20solution%2C%20with%20minimal%20effects%20on%20acid-base%20status%2C%20low%20chloride%20content%2C%20and%20adequate%20tonicity%2C%20is%20not%20yet%20available.%20After%20the%20accumulation%20of%20pre-clinical%20and%20clinical%20physiologic%20data%2C%20in%20the%20last%20three%20years%2C%20several%20clinical%20trials%2C%20mostly%20observational%20and%20retrospective%2C%20have%20addressed%20the%20question%20of%20whether%20the%20use%20of%20balanced%20solutions%20has%20beneficial%20effects%20as%20compared%20to%20the%20standard%20of%20care%2C%20sometimes%20even%20suggesting%20an%20improvement%20in%20survival.%20Nonetheless%2C%20the%20first%20large%20randomized%20controlled%20trial%20comparing%20the%20effects%20of%20a%20balanced%20vs.%20unbalanced%20solutions%20on%20renal%20function%20in%20critically-ill%20patients%20%28SPLIT%20trial%2C%20the%200.9%25%20saline%20vs.%20Plasma-Lyte%20148%20for%20Intensive%20Care%20Unit%20Fluid%20Therapy%29%2C%20just%20recently%20published%2C%20showed%20identical%20equipoise%20between%20the%20two%20treatments.%20In%20the%20present%20review%2C%20we%20offer%20a%20comprehensive%20and%20updated%20summary%20on%20this%20issue%2C%20firstly%2C%20by%20providing%20a%20full%20physiological%20background%20of%20balanced%20solutions%3B%20secondly%2C%20by%20summarizing%20their%20potential%20pathophysiologic%20effects%3B%20and%20lastly%2C%20by%20presenting%20the%20clinical%20evidence%20available%20to%20support%20their%20use%20at%20the%20present%20time.%22%2C%22date%22%3A%222015-12-29%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.5603%5C%2FAIT.a2015.0079%22%2C%22ISSN%22%3A%221731-2531%2C%201642-5758%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fjournals.viamedica.pl%5C%2Fanaesthesiology_intensivetherapy%5C%2Farticle%5C%2Fview%5C%2F43663%22%2C%22collections%22%3A%5B%22KMIJV538%22%5D%2C%22dateModified%22%3A%222019-10-28T07%3A03%3A22Z%22%7D%7D%2C%7B%22key%22%3A%22Q9GQIVLB%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Berkes%20et%20al.%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BBerkes%2C%20Z.%20%26lt%3Bi%26gt%3Bet%20al.%26lt%3B%5C%2Fi%26gt%3B%20MODE-SWITCHING%20IN%20AIR%20TRAFFIC%20CONTROL.%2088.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22MODE-SWITCHING%20IN%20AIR%20TRAFFIC%20CONTROL%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Zs%5Cu00f3fi%22%2C%22lastName%22%3A%22Berkes%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Miguel%22%2C%22lastName%22%3A%22Aulet%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Marc%22%2C%22lastName%22%3A%22Baumgartner%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Roderick%22%2C%22lastName%22%3A%22van%20Dam%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Maria%22%2C%22lastName%22%3A%22Kovacova%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Tony%22%2C%22lastName%22%3A%22Licu%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Cormac%22%2C%22lastName%22%3A%22Russell%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%22%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-10-28T05%3A45%3A55Z%22%7D%7D%2C%7B%22key%22%3A%22L88TQXWY%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Standards%20Association%20of%20Australia%20and%20Standards%20New%20Zealand%22%2C%22parsedDate%22%3A%221996%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BStandards%20Association%20of%20Australia%20%26amp%3B%20Standards%20New%20Zealand.%20%26lt%3Bi%26gt%3BUser-applied%20labels%20for%20use%20on%20syringes%20containing%20drugs%20used%20during%20anaesthesia.%26lt%3B%5C%2Fi%26gt%3B%20%28Standards%20Australia%26%23x202F%3B%3B%20Standards%20New%20Zealand%2C%201996%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22book%22%2C%22title%22%3A%22User-applied%20labels%20for%20use%20on%20syringes%20containing%20drugs%20used%20during%20anaesthesia.%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Standards%20Association%20of%20Australia%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22name%22%3A%22Standards%20New%20Zealand%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%221996%22%2C%22language%22%3A%22en%22%2C%22ISBN%22%3A%22978-0-7337-0404-8%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%224TK53P7R%22%5D%2C%22dateModified%22%3A%222019-10-28T05%3A43%3A40Z%22%7D%7D%2C%7B%22key%22%3A%22JF36U9BU%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Dellamonica%20et%20al.%22%2C%22parsedDate%22%3A%222004%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BDellamonica%2C%20J.%2C%20Boisseau%2C%20N.%2C%20Goubaux%2C%20B.%20%26amp%3B%20Raucoules-Aim%26%23xE9%3B%2C%20M.%20Comparison%20of%20manufacturers%26%23x2019%3B%20specifications%20for%2044%20types%20of%20heat%20and%20moisture%20exchanging%20filters.%20%26lt%3Bi%26gt%3BBritish%20Journal%20of%20Anaesthesia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B93%26lt%3B%5C%2Fb%26gt%3B%2C%20532%26%23x2013%3B539%20%282004%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Comparison%20of%20manufacturers%5Cu2019%20specifications%20for%2044%20types%20of%20heat%20and%20moisture%20exchanging%20filters%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22J.%22%2C%22lastName%22%3A%22Dellamonica%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22N.%22%2C%22lastName%22%3A%22Boisseau%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22B.%22%2C%22lastName%22%3A%22Goubaux%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22M.%22%2C%22lastName%22%3A%22Raucoules-Aim%5Cu00e9%22%7D%5D%2C%22abstractNote%22%3A%22Background.%20Although%20heat%20and%20moisture%20exchanging%20%5Cufb01lters%20%28HMEF%29%20are%20recommended%20for%20use%20during%20anaesthesia%2C%20the%20criteria%20for%20choosing%20a%20%5Cufb01lter%20are%20not%20clearly%20de%5Cufb01ned.%20Manufacturers%20offer%20many%20different%20types%20of%20HMEF%20with%20various%20technical%20characteristics.%20We%20compared%20the%20technical%20speci%5Cufb01cations%20provided%20by%20the%20manufacturers%20for%20different%20types%20of%20HMEF.%5CnMethods.%20Filter%20manufacturers%20were%20asked%20to%20provide%20technical%20information.%20Additional%20information%20was%20obtained%20from%20websites.%20Information%20about%2044%20%5Cufb01lters%20%2816%20mechanical%20and%2028%20electrostatic%29%20was%20collated.%5CnResults.%20Filter%20performances%20were%20estimated%20with%20different%20sizes%20of%20microorganism%20and%20durations%20of%20challenge.%20Twenty-eight%20%5Cufb01lters%20had%20not%20been%20tested%20by%20independent%20laboratories.%20For%2012%20of%20the%20%5Cufb01lters%2C%20information%20obtained%20from%20websites%20and%20from%20the%20manufacturers%20differed.%20Most%20%5Cufb01lter%20speci%5Cufb01cations%20claimed%20high%20ef%5Cufb01ciency%2C%20particularly%20for%20%5Cufb01ltration%2C%20microbial%20challenge%20number%20and%20test%20duration.%20Electrostatic%20%5Cufb01lters%20used%20in%20anaesthesia%20were%20claimed%20to%20have%20high%20%5Cufb01ltration%20ef%5Cufb01ciency%2C%20similar%20to%20the%20ef%5Cufb01ciency%20provided%20by%20mechanical%20%5Cufb01lters.%20Excluding%20moisture%20output%20values%20did%20not%20alter%20the%20general%20conclusions.%5CnConclusions.%20Technical%20aspects%20of%20the%20tests%2C%20international%20standards%2C%20and%20independent%20validation%20should%20be%20considered%20when%20a%20%5Cufb01lter%20is%20chosen.%22%2C%22date%22%3A%2210%5C%2F2004%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1093%5C%2Fbja%5C%2Faeh239%22%2C%22ISSN%22%3A%2200070912%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Flinkinghub.elsevier.com%5C%2Fretrieve%5C%2Fpii%5C%2FS000709121735849X%22%2C%22collections%22%3A%5B%22X8ZVJS4A%22%5D%2C%22dateModified%22%3A%222019-10-28T05%3A05%3A36Z%22%7D%7D%2C%7B%22key%22%3A%22SMJHHY8B%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Frankenfield%22%2C%22parsedDate%22%3A%222010%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BFrankenfield%2C%20D.%20C.%20On%20heat%2C%20respiration%2C%20and%20calorimetry.%20%26lt%3Bi%26gt%3BNutrition%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B26%26lt%3B%5C%2Fb%26gt%3B%2C%20939%26%23x2013%3B950%20%282010%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22On%20heat%2C%20respiration%2C%20and%20calorimetry%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22David%20C.%22%2C%22lastName%22%3A%22Frankenfield%22%7D%5D%2C%22abstractNote%22%3A%22The%20technique%20of%20indirect%20calorimetry%20developed%20with%20the%20sciences%20of%20nutrition%20and%20physiology%20over%20the%20course%20of%20hundreds%20of%20years.%20It%20was%20in%20fact%20fundamental%20to%20the%20establishment%20of%20these%20disciplines.%20This%20review%20describes%20the%20development%20of%20the%20technology%20and%20the%20principles%20of%20body%20function%20it%20has%20revealed.%22%2C%22date%22%3A%2210%5C%2F2010%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.nut.2010.01.002%22%2C%22ISSN%22%3A%2208999007%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Flinkinghub.elsevier.com%5C%2Fretrieve%5C%2Fpii%5C%2FS0899900710000286%22%2C%22collections%22%3A%5B%22KMIJV538%22%5D%2C%22dateModified%22%3A%222019-10-28T04%3A48%3A56Z%22%7D%7D%2C%7B%22key%22%3A%22X4WCTH65%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Wears%20and%20Hettinger%22%2C%22parsedDate%22%3A%222014%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BWears%2C%20R.%20L.%20%26amp%3B%20Hettinger%2C%20A.%20Z.%20The%20Tragedy%20of%20Adaptability.%20%26lt%3Bi%26gt%3BAnnals%20of%20Emergency%20Medicine%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B63%26lt%3B%5C%2Fb%26gt%3B%2C%20338%26%23x2013%3B339%20%282014%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22The%20Tragedy%20of%20Adaptability%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Robert%20L.%22%2C%22lastName%22%3A%22Wears%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A.%20Zachary%22%2C%22lastName%22%3A%22Hettinger%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2203%5C%2F2014%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.annemergmed.2013.10.035%22%2C%22ISSN%22%3A%2201960644%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Flinkinghub.elsevier.com%5C%2Fretrieve%5C%2Fpii%5C%2FS0196064413015540%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%2C%22NS2SUBZA%22%5D%2C%22dateModified%22%3A%222019-10-28T04%3A38%3A35Z%22%7D%7D%2C%7B%22key%22%3A%222IAJ775D%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Webster%20et%20al.%22%2C%22parsedDate%22%3A%222001%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BWebster%2C%20C.%20S.%2C%20Merry%2C%20A.%20F.%2C%20Larsson%2C%20L.%2C%20McGrath%2C%20K.%20A.%20%26amp%3B%20Weller%2C%20J.%20The%20Frequency%20and%20Nature%20of%20Drug%20Administration%20Error%20during%20Anaesthesia.%20%26lt%3Bi%26gt%3BAnaesthesia%20and%20Intensive%20Care%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B29%26lt%3B%5C%2Fb%26gt%3B%2C%20494%26%23x2013%3B500%20%282001%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22The%20Frequency%20and%20Nature%20of%20Drug%20Administration%20Error%20during%20Anaesthesia%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22C.%20S.%22%2C%22lastName%22%3A%22Webster%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A.%20F.%22%2C%22lastName%22%3A%22Merry%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22L.%22%2C%22lastName%22%3A%22Larsson%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22K.%20A.%22%2C%22lastName%22%3A%22McGrath%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22J.%22%2C%22lastName%22%3A%22Weller%22%7D%5D%2C%22abstractNote%22%3A%22We%20aimed%20to%20establish%20the%20frequency%20and%20nature%20of%20drug%20administration%20error%20in%20anaesthesia%20%28a%20significant%20subset%20of%20error%20in%20medicine%29%20at%20two%20hospitals.%20Anaesthetists%20were%20asked%20to%20return%20a%20study%20form%20anonymously%20for%20every%20anaesthetic%2C%20indicating%20whether%20or%20not%20a%20drug%20administration%20error%20or%20pre-error%20%28defined%20as%20any%20incident%20with%20potential%20to%20become%20an%20error%29%20had%20occurred.%20Further%20details%20were%20sought%20if%20the%20response%20was%20affirmative.%22%2C%22date%22%3A%2210%5C%2F2001%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1177%5C%2F0310057X0102900508%22%2C%22ISSN%22%3A%220310-057X%2C%201448-0271%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fjournals.sagepub.com%5C%2Fdoi%5C%2F10.1177%5C%2F0310057X0102900508%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-09-28T06%3A41%3A54Z%22%7D%7D%2C%7B%22key%22%3A%22R3RWHQFS%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Ogawa%20et%20al.%22%2C%22parsedDate%22%3A%222018-01-01%22%2C%22numChildren%22%3A2%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BOgawa%2C%20Y.%2C%20Abe%2C%20K.%2C%20Sakoda%2C%20A.%2C%20Onizuka%2C%20H.%20%26amp%3B%20Sakai%2C%20S.%20FDG-PET%20and%20CT%20findings%20of%20activated%20brown%20adipose%20tissue%20in%20a%20patient%20with%20paraganglioma.%20%26lt%3Bi%26gt%3BEuropean%20Journal%20of%20Radiology%20Open%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B5%26lt%3B%5C%2Fb%26gt%3B%2C%20126%26%23x2013%3B130%20%282018%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22FDG-PET%20and%20CT%20findings%20of%20activated%20brown%20adipose%20tissue%20in%20a%20patient%20with%20paraganglioma%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Yuko%22%2C%22lastName%22%3A%22Ogawa%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Koichiro%22%2C%22lastName%22%3A%22Abe%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Akiko%22%2C%22lastName%22%3A%22Sakoda%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Hiromi%22%2C%22lastName%22%3A%22Onizuka%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Shuji%22%2C%22lastName%22%3A%22Sakai%22%7D%5D%2C%22abstractNote%22%3A%22A%2017-year-old%20female%20had%20been%20complaining%20of%20a%20headache%20for%206%20years.%20She%20presented%20severe%20hypertension%20%28200%5C%2F138%5Cu2009mmHg%29%20on%20admission.%20CT%20showed%20a%20hypervascular%20tumor%20behind%20the%20urinary%20bladder%20and%20a%20swelling%20of%20the%20right%20internal%20obturator%20node.%20Intense%20FDG%20uptakes%20were%20identified%20in%20the%20both%20lesions.%20High%20FDG%20accumulation%20was%20also%20observed%20in%20the%20brown%20adipose%20tissue%20%28BAT%29%20throughout%20the%20patient%26%23039%3Bs%20body%2C%20and%20intense%20contrast%20enhancement%20was%20found%20in%20the%20BAT%20on%20CT.%20The%20diagnosis%20was%20a%20malignant%20paraganglioma%20with%20obturator%20node%20metastasis.%20The%20post-surgery%20FDG-PET%5C%2F%20CT%20examination%20revealed%20that%20the%20FDG%20accumulations%20in%20the%20BAT%20had%20completely%20disappeared.%22%2C%22date%22%3A%22January%201%2C%202018%22%2C%22language%22%3A%22%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.ejro.2018.08.002%22%2C%22ISSN%22%3A%222352-0477%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fwww.sciencedirect.com%5C%2Fscience%5C%2Farticle%5C%2Fpii%5C%2FS2352047718300728%22%2C%22collections%22%3A%5B%22KMIJV538%22%5D%2C%22dateModified%22%3A%222019-09-01T23%3A58%3A55Z%22%7D%7D%2C%7B%22key%22%3A%225B7VCJWH%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BHuman%20brown%20adipose%20tissue%20detected%20by%20fluorodeoxyglucose...%20%26lt%3Bi%26gt%3BResearchGate%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Ba%20class%3D%26%23039%3Bzp-ItemURL%26%23039%3B%20href%3D%26%23039%3Bhttps%3A%5C%2F%5C%2Fwww.researchgate.net%5C%2Ffigure%5C%2FHuman-brown-adipose-tissue-detected-by-fluorodeoxyglucose-FDG-positron-emission_fig2_235730605%26%23039%3B%26gt%3Bhttps%3A%5C%2F%5C%2Fwww.researchgate.net%5C%2Ffigure%5C%2FHuman-brown-adipose-tissue-detected-by-fluorodeoxyglucose-FDG-positron-emission_fig2_235730605%26lt%3B%5C%2Fa%26gt%3B.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22webpage%22%2C%22title%22%3A%22Human%20brown%20adipose%20tissue%20detected%20by%20fluorodeoxyglucose...%22%2C%22creators%22%3A%5B%5D%2C%22abstractNote%22%3A%22Download%20scientific%20diagram%20%7C%20Human%20brown%20adipose%20tissue%20detected%20by%20fluorodeoxyglucose%20%28FDG%29-positron%20emission%20tomography%20%28PET%29.%20FDG%20uptake%20into%20adipose%20tissue%20at%20the%20supraclavicular%20and%20paraspinal%20regions%20is%20detected%20by%20PET.%20The%20FDG%20uptake%20into%20adipose%20tissues%20is%20negligible%20under%20a%20warm%20condition%20at%2027%5Cu2103%20%28A%29%2C%20but%20increases%20greatly%20after%20exposure%20to%20cold%20at%2019%5Cu2103%20%28B%29%20for%202%20hours.%20from%20publication%3A%20Brown%20Adipose%20Tissue%20as%20a%20Regulator%20of%20Energy%20Expenditure%20and%20Body%20Fat%20in%20Humans%20%7C%20Brown%20adipose%20tissue%20%28BAT%29%20is%20recognized%20as%20the%20major%20site%20of%20sympathetically%20activated%20nonshivering%20thermogenesis%20during%20cold%20exposure%20and%20after%20spontaneous%20hyperphagia%2C%20thereby%20controling%20whole-body%20energy%20expenditure%20and%20body%20fat.%20In%20adult%20humans%2C%20BAT%20has%20long%20been...%20%7C%20Energy%20Expenditure%2C%20Brown%20Adipose%20Tissue%20and%20Adipose%20Tissue%20%7C%20ResearchGate%2C%20the%20professional%20network%20for%20scientists.%22%2C%22date%22%3A%22%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.researchgate.net%5C%2Ffigure%5C%2FHuman-brown-adipose-tissue-detected-by-fluorodeoxyglucose-FDG-positron-emission_fig2_235730605%22%2C%22language%22%3A%22en%22%2C%22collections%22%3A%5B%22KMIJV538%22%5D%2C%22dateModified%22%3A%222019-09-01T23%3A48%3A18Z%22%7D%7D%2C%7B%22key%22%3A%22UB92K7XK%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Boon%20and%20van%20Marken%20Lichtenbelt%22%2C%22parsedDate%22%3A%222016%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BBoon%2C%20M.%20R.%20%26amp%3B%20van%20Marken%20Lichtenbelt%2C%20W.%20D.%20Brown%20Adipose%20Tissue%3A%20A%20Human%20Perspective.%20%26lt%3Bi%26gt%3BHandb%20Exp%20Pharmacol%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B233%26lt%3B%5C%2Fb%26gt%3B%2C%20301%26%23x2013%3B319%20%282016%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Brown%20Adipose%20Tissue%3A%20A%20Human%20Perspective%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Mari%5Cu00ebtte%20R.%22%2C%22lastName%22%3A%22Boon%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Wouter%20D.%22%2C%22lastName%22%3A%22van%20Marken%20Lichtenbelt%22%7D%5D%2C%22abstractNote%22%3A%22Since%202009%2C%20the%20presence%20of%20brown%20adipose%20tissue%20%28BAT%29%20in%20adult%20humans%20has%20been%20irrefutably%20proven.%20It%20is%20estimated%20that%20active%20BAT%20can%20contribute%20up%20to%202.5-5%25%20of%20resting%20metabolic%20rate%20in%20humans%2C%20suggesting%20that%20sustained%20activation%20of%20BAT%20may%20alleviate%20obesity%20and%20associated%20disorders.%20In%20the%20current%20chapter%2C%20the%20discovery%20of%20BAT%20in%20adult%20humans%20will%20be%20discussed.%20Furthermore%2C%20the%20characteristics%20of%20human%20BAT%2C%20methods%20to%20visualize%20the%20tissue%20as%20well%20as%20physiological%20and%20pharmacological%20methods%20to%20enhance%20its%20activity%20will%20be%20stressed.%22%2C%22date%22%3A%222016%22%2C%22language%22%3A%22eng%22%2C%22DOI%22%3A%2210.1007%5C%2F164_2015_11%22%2C%22ISSN%22%3A%220171-2004%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22KMIJV538%22%5D%2C%22dateModified%22%3A%222019-09-01T23%3A46%3A02Z%22%7D%7D%2C%7B%22key%22%3A%225YXTP63W%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Frankenfield%22%2C%22parsedDate%22%3A%222010%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BFrankenfield%2C%20D.%20C.%20On%20heat%2C%20respiration%2C%20and%20calorimetry.%20%26lt%3Bi%26gt%3BNutrition%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B26%26lt%3B%5C%2Fb%26gt%3B%2C%20939%26%23x2013%3B950%20%282010%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22On%20heat%2C%20respiration%2C%20and%20calorimetry%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22David%20C.%22%2C%22lastName%22%3A%22Frankenfield%22%7D%5D%2C%22abstractNote%22%3A%22The%20technique%20of%20indirect%20calorimetry%20developed%20with%20the%20sciences%20of%20nutrition%20and%20physiology%20over%20the%20course%20of%20hundreds%20of%20years.%20It%20was%20in%20fact%20fundamental%20to%20the%20establishment%20of%20these%20disciplines.%20This%20review%20describes%20the%20development%20of%20the%20technology%20and%20the%20principles%20of%20body%20function%20it%20has%20revealed.%22%2C%22date%22%3A%2210%5C%2F2010%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.nut.2010.01.002%22%2C%22ISSN%22%3A%2208999007%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Flinkinghub.elsevier.com%5C%2Fretrieve%5C%2Fpii%5C%2FS0899900710000286%22%2C%22collections%22%3A%5B%22KMIJV538%22%5D%2C%22dateModified%22%3A%222019-09-01T10%3A55%3A53Z%22%7D%7D%2C%7B%22key%22%3A%22VX9GLYVR%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Kaiyala%22%2C%22parsedDate%22%3A%222014%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BKaiyala%2C%20K.%20J.%20What%20does%20indirect%20calorimetry%20really%20tell%20us%3F%20%26lt%3Bi%26gt%3BMolecular%20Metabolism%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B3%26lt%3B%5C%2Fb%26gt%3B%2C%20340%26%23x2013%3B341%20%282014%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22What%20does%20indirect%20calorimetry%20really%20tell%20us%3F%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Karl%20J.%22%2C%22lastName%22%3A%22Kaiyala%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2207%5C%2F2014%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1016%5C%2Fj.molmet.2014.03.005%22%2C%22ISSN%22%3A%2222128778%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Flinkinghub.elsevier.com%5C%2Fretrieve%5C%2Fpii%5C%2FS2212877814000726%22%2C%22collections%22%3A%5B%22KMIJV538%22%5D%2C%22dateModified%22%3A%222019-09-01T10%3A53%3A46Z%22%7D%7D%2C%7B%22key%22%3A%22GXR23Y4J%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Shultz%20et%20al.%22%2C%22parsedDate%22%3A%222010%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BShultz%2C%20J.%20%26lt%3Bi%26gt%3Bet%20al.%26lt%3B%5C%2Fi%26gt%3B%20Standardizing%20anesthesia%20medication%20drawers%20using%20human%20factors%20and%20quality%20assurance%20methods.%20%26lt%3Bi%26gt%3BCanadian%20Journal%20of%20Anesthesia%5C%2FJournal%20canadien%20d%26%23x2019%3Banesth%26%23xE9%3Bsie%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B57%26lt%3B%5C%2Fb%26gt%3B%2C%20490%26%23x2013%3B499%20%282010%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Standardizing%20anesthesia%20medication%20drawers%20using%20human%20factors%20and%20quality%20assurance%20methods%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jonas%22%2C%22lastName%22%3A%22Shultz%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jan%20M.%22%2C%22lastName%22%3A%22Davies%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jeff%22%2C%22lastName%22%3A%22Caird%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Susan%22%2C%22lastName%22%3A%22Chisholm%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Karen%22%2C%22lastName%22%3A%22Ruggles%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Raymond%22%2C%22lastName%22%3A%22Puls%22%7D%5D%2C%22abstractNote%22%3A%22Purpose%20In%20Calgary%2C%20each%20of%20the%20three%20acute-care%20adult%20hospitals%20had%20different%20anesthetic%20medication%20carts%20with%20their%20own%20type%20and%20layout%20of%20anesthetic%20medications.%20A%20number%20of%20anesthesiologists%20moved%20among%20the%20different%20sites%2C%20increasing%20the%20potential%20for%20medication%20errors.%20The%20objective%20of%20this%20study%20was%20to%20identify%20the%20anesthetic%20medications%20to%20include%20and%20to%20determine%20how%20they%20should%20be%20grouped%20and%20positioned%20in%20a%20standardized%20anesthesia%20medication%20cart%20drawer.%22%2C%22date%22%3A%225%5C%2F2010%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1007%5C%2Fs12630-010-9274-8%22%2C%22ISSN%22%3A%220832-610X%2C%201496-8975%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Flink.springer.com%5C%2F10.1007%5C%2Fs12630-010-9274-8%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-07-19T11%3A25%3A16Z%22%7D%7D%2C%7B%22key%22%3A%229AIU453C%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Mostert%20and%20R%20Coetzee%22%2C%22parsedDate%22%3A%222014-09-03%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BMostert%2C%20L.%20%26amp%3B%20R%20Coetzee%2C%20A.%20Central%20oxygen%20pipeline%20failure.%20%26lt%3Bi%26gt%3BSouthern%20African%20Journal%20of%20Anaesthesia%20and%20Analgesia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B20%26lt%3B%5C%2Fb%26gt%3B%2C%20214%26%23x2013%3B217%20%282014%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Central%20oxygen%20pipeline%20failure%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Lelan%5Cu00e8%22%2C%22lastName%22%3A%22Mostert%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Andr%5Cu00e9%22%2C%22lastName%22%3A%22R%20Coetzee%22%7D%5D%2C%22abstractNote%22%3A%22Anaesthetic%20and%20critical%20care%20staff%20play%20a%20governing%20role%20in%20the%20comprehension%20of%20a%20hospital%5Cu2019s%20oxygen%20delivery%20system%20and%20associated%20contingency%20plans%20for%20internal%20disaster%20management.%20Therefore%2C%20staff%20must%20be%20thoroughly%20prepared%20and%20properly%20trained%20to%20support%20an%20institution-wide%20emergency%20response%20in%20the%20event%20of%20central%20oxygen%20pipeline%20failure.%22%2C%22date%22%3A%222014-09-03%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1080%5C%2F22201181.2014.979636%22%2C%22ISSN%22%3A%222220-1181%2C%202220-1173%22%2C%22url%22%3A%22https%3A%5C%2F%5C%2Fwww.tandfonline.com%5C%2Fdoi%5C%2Ffull%5C%2F10.1080%5C%2F22201181.2014.979636%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-06-23T10%3A46%3A26Z%22%7D%7D%2C%7B%22key%22%3A%22LVJXHFNM%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Schumacher%20et%20al.%22%2C%22parsedDate%22%3A%222004-01-01%22%2C%22numChildren%22%3A2%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BSchumacher%2C%20S.%20D.%2C%20Brockwell%2C%20R.%20C.%2C%20Andrews%2C%20J.%20J.%20%26amp%3B%20Ogles%2C%20D.%20Bulk%20Liquid%20Oxygen%20Supply%20Failure.%20%26lt%3Bi%26gt%3BAnesthes%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B100%26lt%3B%5C%2Fb%26gt%3B%2C%20186%26%23x2013%3B189%20%282004%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Bulk%20Liquid%20Oxygen%20Supply%20Failure%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Shawn%20D.%22%2C%22lastName%22%3A%22Schumacher%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Russell%20C.%22%2C%22lastName%22%3A%22Brockwell%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22J.%20Jeffrey%22%2C%22lastName%22%3A%22Andrews%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Duane%22%2C%22lastName%22%3A%22Ogles%22%7D%5D%2C%22abstractNote%22%3A%22%2A%20Anesthesiology%20Resident%2C%20%5Cu2021%20Professor%20and%20Vice-Chair%20for%20Education%2C%20University%20of%20Alabama%20School%20of%20Medicine.%20%5Cu2020%20Assistant%20Professor%2C%20University%20of%20Alabama%20School%20of%20Medicine%2C%20Chief%20of%20Anesthesiology%2C%20Birmingham%20Veterans%20Affairs%20Medical%20Center%2C%20Birmingham%2C%20Alabama.%20%5Cu00a7%20Engineering%20Manager%2C%20University%20of%20Alabama%20Hospital%2C%20Department%20of%20Building%20and%20Engineering%20Services%2C%20Birmingham%2C%20Alabama.%20Received%20...%22%2C%22date%22%3A%222004%5C%2F01%5C%2F01%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%220003-3022%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fanesthesiology.pubs.asahq.org%5C%2Farticle.aspx%3Farticleid%3D1943016%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-06-23T10%3A45%3A15Z%22%7D%7D%2C%7B%22key%22%3A%22KE3RZGW6%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Wilkes%22%2C%22parsedDate%22%3A%222002%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BWilkes%2C%20A.%20R.%20Measuring%20the%20filtration%20performance%20of%20breathing%20system%20filters%20using%20sodium%20chloride%20particles.%207%20%282002%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Measuring%20the%20filtration%20performance%20of%20breathing%20system%20filters%20using%20sodium%20chloride%20particles%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22A%20R%22%2C%22lastName%22%3A%22Wilkes%22%7D%5D%2C%22abstractNote%22%3A%22The%20filtration%20performance%20of%2033%20breathing%20system%20filters%20%28nine%20pleated%20hydrophobic%20and%2024%20electrostatic%20filters%29%20was%20measured%20using%20sodium%20chloride%20particles.%20The%20particles%20had%20a%20size%20distribution%20with%20a%20count%20median%20diameter%20of%200.07%20mm%20and%20a%20geometric%20standard%20deviation%20not%20exceeding%201.83.%20The%20geometric%20mean%20penetration%20values%20ranged%20from%200.002%20to%200.67%25%20for%20the%20nine%20pleated%20hydrophobic%20filters%20and%20from%200.25%20to%2035%25%20for%20the%2024%20electrostatic%20filters%20%28p%20%2C%200.0001%20for%20the%20difference%20between%20the%20two%20filter%20types%29.%20The%20filtration%20performance%20obtained%20when%20filters%20are%20challenged%20with%20either%20sodium%20chloride%20particles%20or%20microbes%20is%20compared%20and%20discussed.%22%2C%22date%22%3A%222002%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22X8ZVJS4A%22%5D%2C%22dateModified%22%3A%222019-06-16T23%3A35%3A24Z%22%7D%7D%2C%7B%22key%22%3A%2233G5B2FS%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Merry%20and%20Webster%22%2C%22parsedDate%22%3A%222008%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BMerry%2C%20A.%20F.%20%26amp%3B%20Webster%2C%20C.%20S.%20Medication%20error%20in%20New%20Zealand%26%23x2014%3Btime%20to%20act.%20%26lt%3Bb%26gt%3B121%26lt%3B%5C%2Fb%26gt%3B%2C%205%20%282008%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Medication%20error%20in%20New%20Zealand%5Cu2014time%20to%20act%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Alan%20F%22%2C%22lastName%22%3A%22Merry%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Craig%20S%22%2C%22lastName%22%3A%22Webster%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222008%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%22%22%2C%22ISSN%22%3A%22%22%2C%22url%22%3A%22%22%2C%22collections%22%3A%5B%22ICHFBI3J%22%5D%2C%22dateModified%22%3A%222019-04-18T06%3A32%3A27Z%22%7D%7D%2C%7B%22key%22%3A%22T9SI3WZL%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Asai%20et%20al.%22%2C%22parsedDate%22%3A%222000-06-15%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BAsai%2C%20T.%2C%20Matsumoto%2C%20S.%20%26amp%3B%20Shingu%2C%20K.%20Incidence%20of%20blood-borne%20infectious%20micro-organisms%3A%20would%20you%20still%20not%20wear%20gloves%3F%20%26lt%3Bi%26gt%3BAnaesthesia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B55%26lt%3B%5C%2Fb%26gt%3B%2C%20591%26%23x2013%3B592%20%282000%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Incidence%20of%20blood-borne%20infectious%20micro-organisms%3A%20would%20you%20still%20not%20wear%20gloves%3F%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22T.%22%2C%22lastName%22%3A%22Asai%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22S.%22%2C%22lastName%22%3A%22Matsumoto%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22K.%22%2C%22lastName%22%3A%22Shingu%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%222000-06-15%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1046%5C%2Fj.1365-2044.2000.01479-4.x%22%2C%22ISSN%22%3A%2200032409%2C%2013652044%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fdoi.wiley.com%5C%2F10.1046%5C%2Fj.1365-2044.2000.01479-4.x%22%2C%22collections%22%3A%5B%224TK53P7R%22%5D%2C%22dateModified%22%3A%222019-04-01T11%3A45%3A14Z%22%7D%7D%2C%7B%22key%22%3A%22TRTMFMYF%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Marshall%20and%20Chrimes%22%2C%22parsedDate%22%3A%222019%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BMarshall%2C%20S.%20D.%20%26amp%3B%20Chrimes%2C%20N.%20Medication%20handling%3A%20towards%20a%20practical%2C%20human-centred%20approach.%20%26lt%3Bi%26gt%3BAnaesthesia%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B74%26lt%3B%5C%2Fb%26gt%3B%2C%20280%26%23x2013%3B284%20%282019%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Medication%20handling%3A%20towards%20a%20practical%2C%20human-centred%20approach%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22S.%20D.%22%2C%22lastName%22%3A%22Marshall%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22N.%22%2C%22lastName%22%3A%22Chrimes%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22date%22%3A%2203%5C%2F2019%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1111%5C%2Fanae.14482%22%2C%22ISSN%22%3A%2200032409%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fdoi.wiley.com%5C%2F10.1111%5C%2Fanae.14482%22%2C%22collections%22%3A%5B%224TK53P7R%22%5D%2C%22dateModified%22%3A%222019-03-26T05%3A17%3A03Z%22%7D%7D%2C%7B%22key%22%3A%224KN9FITW%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Orser%20et%20al.%22%2C%22parsedDate%22%3A%222001%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BOrser%2C%20B.%20A.%2C%20Chen%2C%20R.%20J.%20B.%20%26amp%3B%20Yee%2C%20D.%20A.%20Medication%20errors%20in%20anesthetic%20practice%3A%20a%20survey%20of%20687%20practitioners.%20%26lt%3Bi%26gt%3BCanadian%20Journal%20of%20Anesthesia%5C%2FJournal%20canadien%20d%26%23x2019%3Banesth%26%23xE9%3Bsie%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B48%26lt%3B%5C%2Fb%26gt%3B%2C%20139%26%23x2013%3B146%20%282001%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22Medication%20errors%20in%20anesthetic%20practice%3A%20a%20survey%20of%20687%20practitioners%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Beverley%20A.%22%2C%22lastName%22%3A%22Orser%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Robert%20J.%20B.%22%2C%22lastName%22%3A%22Chen%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Doreen%20A.%22%2C%22lastName%22%3A%22Yee%22%7D%5D%2C%22abstractNote%22%3A%22Purpose%3A%20The%20objectives%20of%20this%20study%20were%20to%20determine%3A%201%29%20if%20anesthesiologists%20had%20experienced%20a%20medication%20error%20and%202%29%20to%20identify%20causal%20factors.%20The%20perceived%20value%20of%20a%20Canadian%20reporting%20agency%20for%20medication%20errors%20and%20improved%20standards%20for%20labels%20on%20drug%20ampoules%20was%20also%20investigated.%5CnMethods%3A%20A%20self-reporting%20survey%20was%20mailed%20to%20members%20of%20the%20Canadian%20Anesthesiologists%5Cu2019%20Society%20%28n%20%3D%202%2C266%29.%20Respondents%20provided%20free-text%20descriptions%20of%20medication%20errors%20and%20answered%20fixed%20response%20questions.%5CnResults%3A%20Surveys%20from%20687%20anesthesiologists%20%2830%25%20response%20rate%29%20revealed%20that%2085%25%20of%20the%20participants%20had%20experienced%20at%20least%20one%20drug%20error%20or%20%5Cu201cnear%20miss%5Cu201d.%20Although%20most%20errors%20%281%2C038%29%20were%20of%20minor%20consequence%20%2898%25%29%2C%20four%20deaths%20were%20reported.%20The%20commonest%20error%20involved%20the%20administration%20of%20muscle%20relaxants%20instead%20of%20a%20reversal%20agent.%20%5Cu201cSyringe%20swaps%5Cu201d%20%2870.4%25%29%20and%20the%20misidentification%20of%20the%20label%20%2846.8%25%29%20were%20common%20contributing%20factors.%20Anesthesiologists%20%2897.9%25%29%20reported%20that%20they%20read%20the%20ampoule%20label%20%5Cu201cmost%20of%20the%20time%5Cu201d%20although%20the%20label%20colour%20was%20an%20important%20secondary%20cue.%20Approximately%20half%20of%20the%20participants%20would%20report%20the%20error%20if%20a%20reporting%20program%20existed%20and%2084%25%20agreed%20that%20improved%20standards%20for%20drug%20labels%20would%20reduce%20the%20incidence%20of%20error.%5CnConclusions%3A%20Most%20anesthesiologists%20experienced%20at%20least%20one%20drug%20error.%20The%20commonest%20error%20was%20a%20%5Cu201csyringe%20swap%5Cu201d%20that%20involved%20a%20muscle%20relaxant.%20Most%20errors%20were%20of%20minor%20consequence%2C%20however%2C%20serious%20morbidity%20and%20mortality%20resulted%20from%20clearly%20preventable%20events.%20These%20results%20support%20the%20development%20of%20improved%20standards%20for%20drug%20labels%20and%20the%20establishment%20of%20a%20Canadian%20reporting%20program%20for%20medication%20errors.%22%2C%22date%22%3A%222%5C%2F2001%22%2C%22language%22%3A%22en%22%2C%22DOI%22%3A%2210.1007%5C%2FBF03019726%22%2C%22ISSN%22%3A%220832-610X%2C%201496-8975%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Flink.springer.com%5C%2F10.1007%5C%2FBF03019726%22%2C%22collections%22%3A%5B%224TK53P7R%22%5D%2C%22dateModified%22%3A%222019-03-26T05%3A08%3A28Z%22%7D%7D%2C%7B%22key%22%3A%22UFA6W5CC%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Lally%20et%20al.%22%2C%22parsedDate%22%3A%222010-10%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BLally%2C%20P.%2C%20van%20Jaarsveld%2C%20C.%20H.%20M.%2C%20Potts%2C%20H.%20W.%20W.%20%26amp%3B%20Wardle%2C%20J.%20How%20are%20habits%20formed%3A%20Modelling%20habit%20formation%20in%20the%20real%20world.%20%26lt%3Bi%26gt%3BEuropean%20Journal%20of%20Social%20Psychology%26lt%3B%5C%2Fi%26gt%3B%20%26lt%3Bb%26gt%3B40%26lt%3B%5C%2Fb%26gt%3B%2C%20998%26%23x2013%3B1009%20%282010%29.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22journalArticle%22%2C%22title%22%3A%22How%20are%20habits%20formed%3A%20Modelling%20habit%20formation%20in%20the%20real%20world%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Phillippa%22%2C%22lastName%22%3A%22Lally%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Cornelia%20H.%20M.%22%2C%22lastName%22%3A%22van%20Jaarsveld%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Henry%20W.%20W.%22%2C%22lastName%22%3A%22Potts%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Jane%22%2C%22lastName%22%3A%22Wardle%22%7D%5D%2C%22abstractNote%22%3A%22To%20investigate%20the%20process%20of%20habit%20formation%20in%20everyday%20life%2C%2096%20volunteers%20chose%20an%20eating%2C%20drinking%20or%20activity%20behaviour%20to%20carry%20out%20daily%20in%20the%20same%20context%20%28for%20example%20%26%23039%3Bafter%20breakfast%26%23039%3B%29%20for%2012%20weeks.%20They%20completed%20the%20self-report%20habit%20index%20%28SRHI%29%20each%20day%20and%20recorded%20whether%20they%20carried%20out%20the%20behaviour.%20The%20majority%20%2882%29%20of%20participants%20provided%20sufficient%20data%20for%20analysis%2C%20and%20increases%20in%20automaticity%20%28calculated%20with%20a%20sub-set%20of%20SRHI%20items%29%20were%20examined%20over%20the%20study%20period.%20Nonlinear%20regressions%20fitted%20an%20asymptotic%20curve%20to%20each%20individual%26%23039%3Bs%20automaticity%20scores%20over%20the%2084%20days.%20The%20model%20fitted%20for%2062%20individuals%2C%20of%20whom%2039%20showed%20a%20good%20fit.%20Performing%20the%20behaviour%20more%20consistently%20was%20associated%20with%20better%20model%20fit.%20The%20time%20it%20took%20participants%20to%20reach%2095%25%20of%20their%20asymptote%20of%20automaticity%20ranged%20from%2018%20to%20254%20days%3B%20indicating%20considerable%20variation%20in%20how%20long%20it%20takes%20people%20to%20reach%20their%20limit%20of%20automaticity%20and%20highlighting%20that%20it%20can%20take%20a%20very%20long%20time.%20Missing%20one%20opportunity%20to%20perform%20the%20behaviour%20did%20not%20materially%20affect%20the%20habit%20formation%20process.%20With%20repetition%20of%20a%20behaviour%20in%20a%20consistent%20context%2C%20automaticity%20increases%20following%20an%20asymptotic%20curve%20which%20can%20be%20modelled%20at%20the%20individual%20level.%20Copyright%20%5Cu00a9%202009%20John%20Wiley%20%26amp%3B%20Sons%2C%20Ltd.%22%2C%22date%22%3A%22October%202010%22%2C%22language%22%3A%22%22%2C%22DOI%22%3A%2210.1002%5C%2Fejsp.674%22%2C%22ISSN%22%3A%2200462772%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Fezproxy.newcastle.edu.au%5C%2Flogin%3Furl%3Dhttp%3A%5C%2F%5C%2Fsearch.ebscohost.com%5C%2Flogin.aspx%3Fdirect%3Dtrue%26db%3Dpbh%26AN%3D53843531%26site%3Deds-live%22%2C%22collections%22%3A%5B%228Q7C3J32%22%5D%2C%22dateModified%22%3A%222019-03-13T09%3A06%3A28Z%22%7D%7D%2C%7B%22key%22%3A%22JAGBNH6D%22%2C%22library%22%3A%7B%22id%22%3A4088554%7D%2C%22meta%22%3A%7B%22creatorSummary%22%3A%22Gardner%20and%20Rebar%22%2C%22parsedDate%22%3A%222016-08-31%22%2C%22numChildren%22%3A1%7D%2C%22bib%22%3A%22%26lt%3Bdiv%20class%3D%26quot%3Bcsl-bib-body%26quot%3B%20style%3D%26quot%3Bline-height%3A%202%3B%20%26quot%3B%26gt%3B%5Cn%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-entry%26quot%3B%20style%3D%26quot%3Bclear%3A%20left%3B%20%26quot%3B%26gt%3B%5Cn%20%20%20%20%26lt%3Bdiv%20class%3D%26quot%3Bcsl-left-margin%26quot%3B%20style%3D%26quot%3Bfloat%3A%20left%3B%20padding-right%3A%200.5em%3B%20text-align%3A%20right%3B%20width%3A%201em%3B%26quot%3B%26gt%3B1.%26lt%3B%5C%2Fdiv%26gt%3B%26lt%3Bdiv%20class%3D%26quot%3Bcsl-right-inline%26quot%3B%20style%3D%26quot%3Bmargin%3A%200%20.4em%200%201.5em%3B%26quot%3B%26gt%3BGardner%2C%20B.%20%26amp%3B%20Rebar%2C%20A.%20L.%20Habit%20Formation%20and%20Behavior%20Change.%20in%20%26lt%3Bi%26gt%3BOxford%20Research%20Encyclopedia%20of%20Psychology%26lt%3B%5C%2Fi%26gt%3B%20%28Oxford%20University%20Press%2C%202016%29.%20doi%3A10.1093%5C%2Facrefore%5C%2F9780190236557.013.129.%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%20%20%26lt%3B%5C%2Fdiv%26gt%3B%5Cn%26lt%3B%5C%2Fdiv%26gt%3B%22%2C%22data%22%3A%7B%22itemType%22%3A%22bookSection%22%2C%22title%22%3A%22Habit%20Formation%20and%20Behavior%20Change%22%2C%22creators%22%3A%5B%7B%22creatorType%22%3A%22bookAuthor%22%2C%22firstName%22%3A%22Benjamin%22%2C%22lastName%22%3A%22Gardner%22%7D%2C%7B%22creatorType%22%3A%22bookAuthor%22%2C%22firstName%22%3A%22Amanda%20L.%22%2C%22lastName%22%3A%22Rebar%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Benjamin%22%2C%22lastName%22%3A%22Gardner%22%7D%2C%7B%22creatorType%22%3A%22author%22%2C%22firstName%22%3A%22Amanda%20L.%22%2C%22lastName%22%3A%22Rebar%22%7D%5D%2C%22abstractNote%22%3A%22%22%2C%22bookTitle%22%3A%22Oxford%20Research%20Encyclopedia%20of%20Psychology%22%2C%22date%22%3A%222016-08-31%22%2C%22language%22%3A%22en%22%2C%22ISBN%22%3A%22978-0-19-023655-7%22%2C%22url%22%3A%22http%3A%5C%2F%5C%2Foxfordre.com%5C%2Fpsychology%5C%2Fview%5C%2F10.1093%5C%2Facrefore%5C%2F9780190236557.001.0001%5C%2Facrefore-9780190236557-e-129%22%2C%22collections%22%3A%5B%228Q7C3J32%22%5D%2C%22dateModified%22%3A%222019-03-13T09%3A03%3A17Z%22%7D%7D%5D%7D
1.
Rae, A., Provan, D., Aboelssaad, H. & Alexander, R. A manifesto for Reality-based Safety Science. Safety Science 126, 104654 (2020).
1.
Salmon, P. M. et al. The big picture on accident causation: A review, synthesis and meta-analysis of AcciMap studies. Safety Science 126, 104650 (2020).
1.
Zippel, C., Börgers, A., Weitzel, A. & Bohnet-Joschko, S. Many critical incidents could be avoided by preanaesthesia equipment checks: Lessons for high reliability organisations. European Journal of Anaesthesiology 31, 289–291 (2014).
1.
Zippel, C., Borgers, A., Weitzel, A. & Bohnet-Joschko, S. Many critical incidents could be avoided by preanaesthesia equipment checks: Lessons for high reliability organisations. [Letter]. Journal of Anaesthesiology 31, 289–291 (2014).
1.
Wilkes, A. R., Pandit, J. J. & O’Sullivan, E. The history of anaesthetic equipment evaluation in the United Kingdom: lessons for developing future strategy. Anaesthesia 66, 34–39 (2011).
1.
Cook, T. M. et al. Multicentre clinical simulation evaluation of the ISO 80369-6 neuraxial non-Luer connector. Anaesthesia 74, 619–629 (2019).
1.
Cassidy, C. J., Smith, A. & Arnot‐Smith, J. Critical incident reports concerning anaesthetic equipment: analysis of the UK National Reporting and Learning System (NRLS) data from 2006–2008*. Anaesthesia 66, 879–888 (2011).
1.
Checklist for anaesthetic equipment. 2.
1.
Association of Anaesthetists of Great Britain and, Ireland et al. Checking Anaesthetic Equipment 2012: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia 67, 660–668 (2012).
1.
Bourgain, J. L., Coisel, Y., Kern, D., Nouette-Gaulain, K. & Panczer, M. What are the main “machine dysfunctions” to know? Annales Françaises d’Anesthésie et de Réanimation 33, 466–471 (2014).
1.
Orihara, M. Comparison of incidence of anaphylaxis between sugammadex and neostigmine: a retrospective multicentre observational study. 10.
1.
Xie, A. & Carayon, P. A systematic review of human factors and ergonomics (HFE)-based healthcare system redesign for quality of care and patient safety. Ergonomics 58, 33–49 (2015).
1.
Wilkes, A. R. Measuring the filtration performance of breathing system filters using sodium chloride particles. 7 (2002).
1.
Merry, A. F., Shipp, D. H. & Lowinger, J. S. The contribution of labelling to safe medication administration in anaesthetic practice. Best Practice & Research Clinical Anaesthesiology 25, 145–159 (2011).
1.
Shultz, J. et al. Standardizing anesthesia medication drawers using human factors and quality assurance methods. Canadian Journal of Anesthesia/Journal canadien d’anesthésie 57, 490–499 (2010).
1.
Holloway, C. M. & Johnson, C. W. Reducing our ignorance: finding answers to certain epistemic questions for software systems. in
6th IET International Conference on System Safety 2011 D12–D12 (IET, 2011).
http://doi.org/10.1049/cp.2011.0269.
1.
Arthmar, R. VILFREDO PARETO. Manual of Political Economy. A critical and variorum edition. Edited by Aldo Montesano, Alberto Zanni, Luigino Bruni, John Chipman and Michael McLure. Oxford: Oxford University Press, 2014, 664 p. Estudos Econômicos (São Paulo) 45, 459–470 (2015).
1.
Donzelli, F. Pareto’s Mechanical Dream. 47.
1.
Muschara, T. Critical Steps: How to Identify and Manage the Most Important Human Performance Risks in Operations. Performance Improvement 53, 11–21 (2014).
1.
Keijzer, C., Perez, R. S. G. M. & de Lange, J. J. Compound A and carbon monoxide production from sevoflurane and seven different types of carbon dioxide absorbent in a patient model. Acta Anaesthesiologica Scandinavica 51, 31–37 (2007).
1.
Saito, M. Brown Adipose Tissue as a Regulator of Energy Expenditure and Body Fat in Humans. Diabetes & Metabolism Journal 37, 22 (2013).
1.
Razzouk, R. & Shute, V. What Is Design Thinking and Why Is It Important? Review of Educational Research 82, 330–348 (2012).
1.
Lally, P., Potts, H. W. W. & Wardle, J. Research article How are habits formed: Modelling habit formation in the real worldy. Eur. J. Soc. Psychol. 13 (2009).
1.
Catchpole, K., Bell, M. D. D. & Johnson, S. Safety in anaesthesia: a study of 12 606 reported incidents from the UK National Reporting and Learning System. Anaesthesia 63, 340–346 (2008).
1.
Nedergaard, J., Bengtsson, T. & Cannon, B. Unexpected evidence for active brown adipose tissue in adult humans. American Journal of Physiology-Endocrinology and Metabolism 293, E444–E452 (2007).
1.
Kothari, D. & Agrawal, J. Colour-coded syringe labels: a modification to enhance patient safety. British Journal of Anaesthesia 110, 1056–1058 (2013).
1.
Furniss, D., Dean Franklin, B. & Blandford, A. The devil is in the detail: How a closed-loop documentation system for IV infusion administration contributes to and compromises patient safety.
Health Informatics Journal 146045821983957 (2019)
http://doi.org/10.1177/1460458219839574.
1.
Langer, T. et al. Intravenous balanced solutions: from physiology to clinical evidence. Anestezjologia Intensywna Terapia 47, 78–88 (2015).
1.
Berkes, Z. et al. MODE-SWITCHING IN AIR TRAFFIC CONTROL. 88.
1.
Standards Association of Australia & Standards New Zealand. User-applied labels for use on syringes containing drugs used during anaesthesia. (Standards Australia ; Standards New Zealand, 1996).
1.
Dellamonica, J., Boisseau, N., Goubaux, B. & Raucoules-Aimé, M. Comparison of manufacturers’ specifications for 44 types of heat and moisture exchanging filters. British Journal of Anaesthesia 93, 532–539 (2004).
1.
Frankenfield, D. C. On heat, respiration, and calorimetry. Nutrition 26, 939–950 (2010).
1.
Wears, R. L. & Hettinger, A. Z. The Tragedy of Adaptability. Annals of Emergency Medicine 63, 338–339 (2014).
1.
Webster, C. S., Merry, A. F., Larsson, L., McGrath, K. A. & Weller, J. The Frequency and Nature of Drug Administration Error during Anaesthesia. Anaesthesia and Intensive Care 29, 494–500 (2001).
1.
Ogawa, Y., Abe, K., Sakoda, A., Onizuka, H. & Sakai, S. FDG-PET and CT findings of activated brown adipose tissue in a patient with paraganglioma. European Journal of Radiology Open 5, 126–130 (2018).
1.
Boon, M. R. & van Marken Lichtenbelt, W. D. Brown Adipose Tissue: A Human Perspective. Handb Exp Pharmacol 233, 301–319 (2016).
1.
Frankenfield, D. C. On heat, respiration, and calorimetry. Nutrition 26, 939–950 (2010).
1.
Kaiyala, K. J. What does indirect calorimetry really tell us? Molecular Metabolism 3, 340–341 (2014).
1.
Shultz, J. et al. Standardizing anesthesia medication drawers using human factors and quality assurance methods. Canadian Journal of Anesthesia/Journal canadien d’anesthésie 57, 490–499 (2010).
1.
Mostert, L. & R Coetzee, A. Central oxygen pipeline failure. Southern African Journal of Anaesthesia and Analgesia 20, 214–217 (2014).
1.
Schumacher, S. D., Brockwell, R. C., Andrews, J. J. & Ogles, D. Bulk Liquid Oxygen Supply Failure. Anesthes 100, 186–189 (2004).
1.
Wilkes, A. R. Measuring the filtration performance of breathing system filters using sodium chloride particles. 7 (2002).
1.
Merry, A. F. & Webster, C. S. Medication error in New Zealand—time to act. 121, 5 (2008).
1.
Asai, T., Matsumoto, S. & Shingu, K. Incidence of blood-borne infectious micro-organisms: would you still not wear gloves? Anaesthesia 55, 591–592 (2000).
1.
Marshall, S. D. & Chrimes, N. Medication handling: towards a practical, human-centred approach. Anaesthesia 74, 280–284 (2019).
1.
Orser, B. A., Chen, R. J. B. & Yee, D. A. Medication errors in anesthetic practice: a survey of 687 practitioners. Canadian Journal of Anesthesia/Journal canadien d’anesthésie 48, 139–146 (2001).
1.
Lally, P., van Jaarsveld, C. H. M., Potts, H. W. W. & Wardle, J. How are habits formed: Modelling habit formation in the real world. European Journal of Social Psychology 40, 998–1009 (2010).
1.
Gardner, B. & Rebar, A. L. Habit Formation and Behavior Change. in Oxford Research Encyclopedia of Psychology (Oxford University Press, 2016). doi:10.1093/acrefore/9780190236557.013.129.